I have been sharing Sean’s journey out of overtraining syndrome (OTS) since he started working with me , through what his program looked midway to his final recovery week (today).
Unlike other programs that you will find in this coach log, Sean’s program didn’t have a strategy chart with intensity goals according to whatever the general objective is. In Sean’s program, the plan was to progress, along 12 weeks, from very low volume, very low intensity and very low skill challenge to higher volume and higher skill challenge. His feedback and the feedback provided by the physician was crucial for adjusting these variables. Monitoring is necessarily multidimensional.
One thing I haven’t justified here is why I insisted so much on having him identify what type of activity provided him with the greatest pleasure. I have a general dislike for the popularized and scientifically very wrong version of mental toughness according to which training must be painful and unpleasant. I wrote about 40 thousand words on such misconceptions and you can find them here. There is one word about them: wrong. While managing an OTS patient, that goes beyond wrong: it can actually be very harmful.
It is consensual that OTS is related to worsened mood, among other behavioral consequences. It is not uncommon for OTS athletes to be treated for depression and for OTS to go undiagnosed since there is no consensus about diagnosis criteria. A lot has been researched but not enough to say we know what OTS is, how to identify it and how to treat it. The little we know, however, suggests that psychological and social aspects are critical.
That is why my initial conversation with Sean was about what he really enjoyed doing. The off days included biking with his kids and engaging in light, enjoyable physical activity. Approaching his worsened mood was as critical as approaching all the other clinical manifestations of his OTS. Walt didn’t prescribe anti-depressants at first and we agreed to adopt “watchful waiting” in that respect. As Sean’s mood improved in the first 10 days, Walt felt no need to use psychiatric medication.
Deliberately avoiding weights he could easily do for reps, in any lift, was a challenge for Sean and one he was surprised to have handled so well.
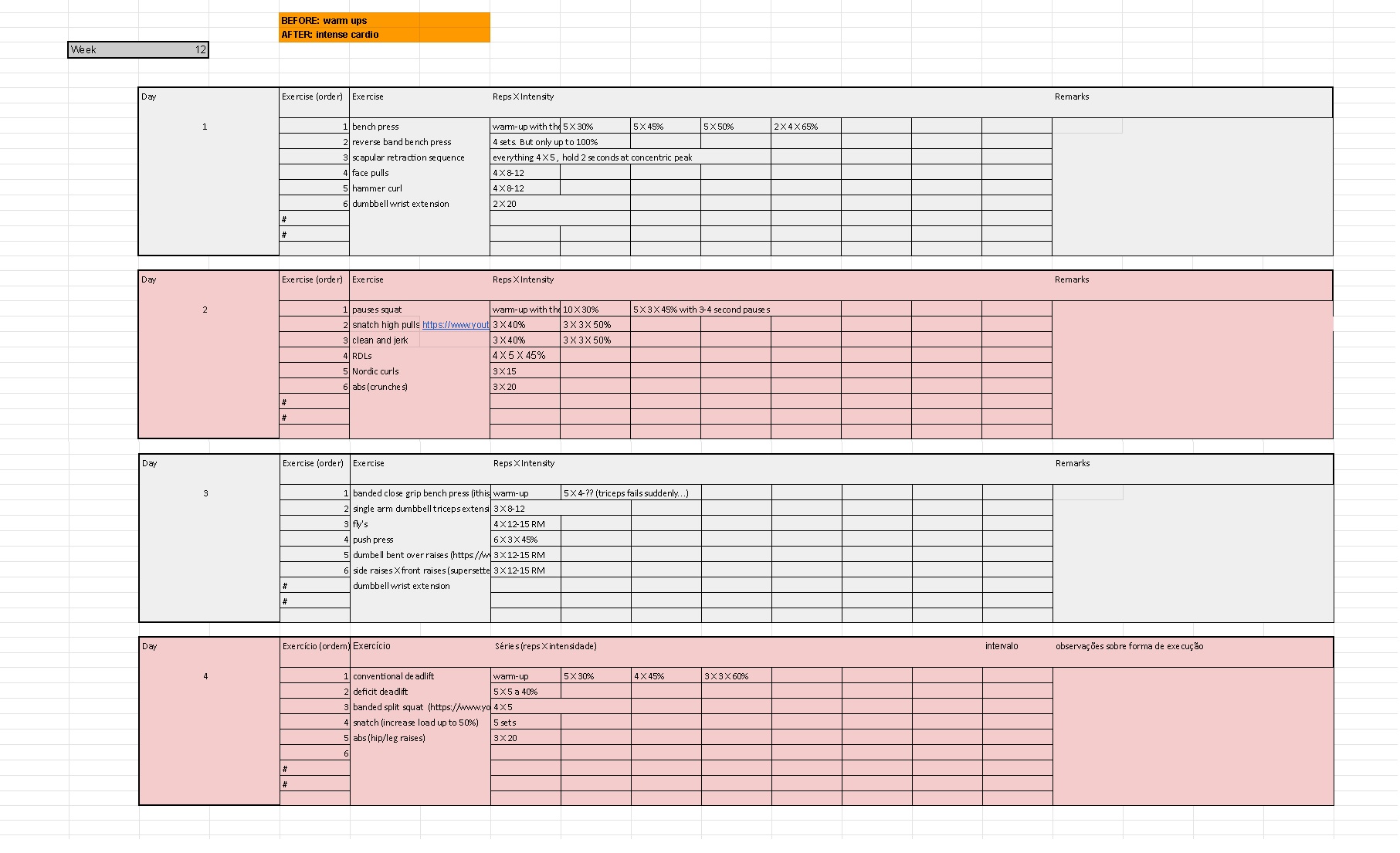
In the last week, I introduced one supra-maximal effort exercise: reverse band bench press. Even then, it was just up to 100% and as a test for the transition into the next cycle. He obviously enjoyed it a lot.
The takeaways from this case are:
- OTS is complex and the symptoms are not consistent. Each case is different and must be treated as such. It’s important for the coach to be aware (different from familiar with) of the science behind it but use it for cautionary decisions rather than guidelines.
- Monitoring the athlete/patient's mental improvement is as critical as his physical improvements such as tolerance for volume, coordination and better conditioning indicators.
- Being able to work with a physician makes all the difference.
- Understand the dangers of exercise deprivation, elaborate a program to prevent that and at the same time avoid excessive physical stimulus. It’s a fine line that the coach must fine-tune to each patient/athlete.
Week 12 - CLICK TO ENLARGE