










Introduction
It doesn’t dawn on aging people because decay is more or less linear until it isn’t, and then it’s too late. It doesn’t dawn on us until reality punches us in the stomach and holds our face into the abyss. As we stare, it stares back at us and finally speaks: either we remain strong and conditioned, to the best of our capacity, until the end, or that end will be shaped by the horrors of chaotic slow decay.
Sooner or later, the reality shock will happen to everyone, whether it is about us or a loved one. The average healthy son or daughter who visits their parents every week, the physician who trusts they have the tools to handle health emergencies, the coach who was introduced to age-related strength and conditioning losses in college but filed that content in some dark corner of the mind, and even the scholar, who actually studied age-related risks and inactivity disorders. It doesn’t matter. It’s too abstract, too far and too impossible.
The great majority of us live in denial of death and decay. It remains the stuff of scholarly writing, journalism or fiction. Our moms and dads, they don't degenerate and most of all, they don't die, says the little voice of the child we once were, forever influencing our perception, behavior, and reactions.
The “forever young” marketing ideal bombards us from the moment we are exposed to a screen. Marketing is a big reinforcement to our denial of aging and death.
Reality doesn’t care about our denial. The truth is that humans are being burdened by the consequences of inactivity, poor nutrition, and unhealthy aging more than ever before.
In 2004, the World Health Organization approved the Global strategy on diet, physical activity and health (WHA57.17). The WHO task force has a long history involving public health data and efforts from several countries. It is the result of a multi-government consensus concerning the health burden of inactivity and poor nutrition with associated world-wide high morbidity and mortality rates. Non-transmissible disorders caused by inactivity and poor nutrition finally superseded infectious diseases as major causes of disease and death. These non-transmissible diseases affect all cohorts but, as expected, as people age, the accumulated damage becomes irreversible and pulverized in a myriad of degenerating processes in the body.
Poverty aggravates the situation, whether in rural and undeveloped countries, through hunger, or in predominantly urban and industrialized countries, with their food deserts and the disruption of traditional social support networks.
Aging equals disease. Or does it? After all, what is aging?
A few decades ago there was great enthusiasm with the evidence about the damaging effects of reactive oxygen species. Aging was, then, “accumulated oxidation”. The next intellectual enthusiasm was with the converging evidence about inflammation. Aging became “accumulated inflammation”. We are now in the age of interactive networks and axes. Mostly, we are in awe about the multitude of effects that gut microbiota imbalances can cause.
Underlying all that is the old concept of homeostasis. What the axes and networks promote is systematic, dynamic and permanently adapting cross-talk between all the organs and functions that keep a eukaryotic multi-cellular organism “healthy”, or in “a state of dynamic equilibrium”.
Only recently, the role of the muscle as an interlocutor in the body’s cross-talk was proposed and is currently the focus of intense research efforts.
Cause-orphan evidence (when we know something exists but we don’t know the mechanisms causing it) concerning the beneficial effect of physical activity on mental and physical health is now making sense. Most of all, the deadly risk of inactivity is making sense as well.
As other forms of physical activity become less realistic for older individuals, strength training takes a prominent role in contributing to the organism’s homeostasis. It is the type of exercise that best and most safely promotes the maintenance of skeletal muscle mass and keeps it contracting. Healthy aging involves deliberate efforts to maintain homeostasis.
In this article, I will introduce explanations about the role of strength and conditioning in healthy living and suggest how we can promote that.
The muscle as a mediator in the body cross-talk
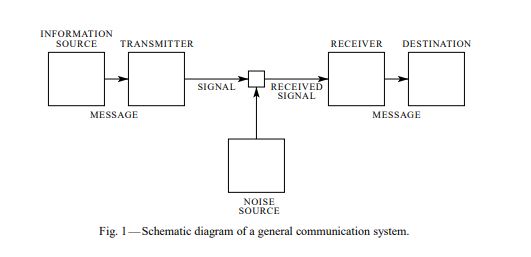
Life evolved through gradual and large evolutionary leaps. Evolution functions through random genetic mutation combined with intra-specific populational selection. A first big challenge was cellular existence. A cell is an incredibly complex cybernetic communication system. The genetic code is a language that generates messages. The messages are received by receptors, interpreted and responded to. All of this happens inside a cell. When eukaryotes became viable – cells with their “central control” genetic material contained in the nucleus, an outside membrane separating the organism from its environment and several organelles – communication became far more complex. As the level of structural complexity changed, so more complex communication systems were selected for. The next big challenge was the leap to multi-cellular life, which is only possible if there is a mechanism by which all individual cells can communicate with one another. The emergence of animals with organs (differentiated cells and tissues) and a nervous system increased the complexity of intracellular, cell-to-cell, inter-organ and inter-organism communication.
Any communication (information transfer) system is made of an information source and a destination. The information source generates the message, a transmitter produces a signal that is received by a receiver and reaches a destination. Throughout the process, there is coding and decoding of the message.
Shannon 1948, Shannon 1998.
Or:
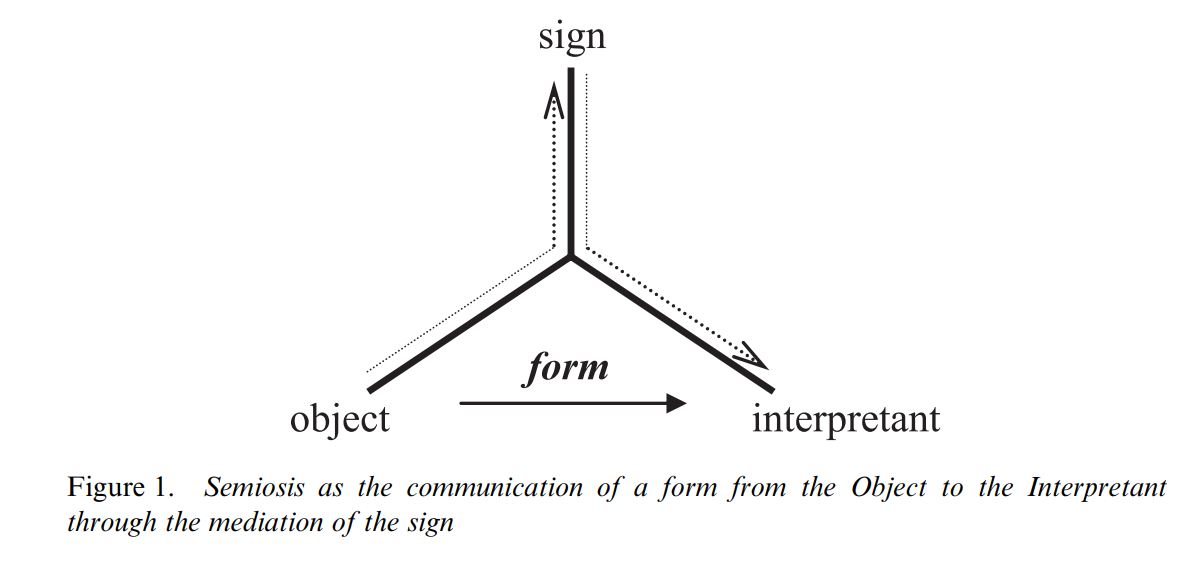
From El-Hani et al 2006
Noise creates ambivalence and ambiguity in the communication system:
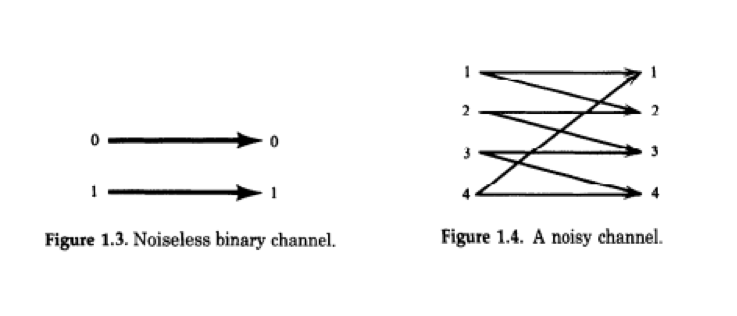 Cover & Thomas 2012.
Cover & Thomas 2012.
When the genetic material was discovered and the genetic code broken, this is what was assumed to be the “dogma” of biological information transfer:
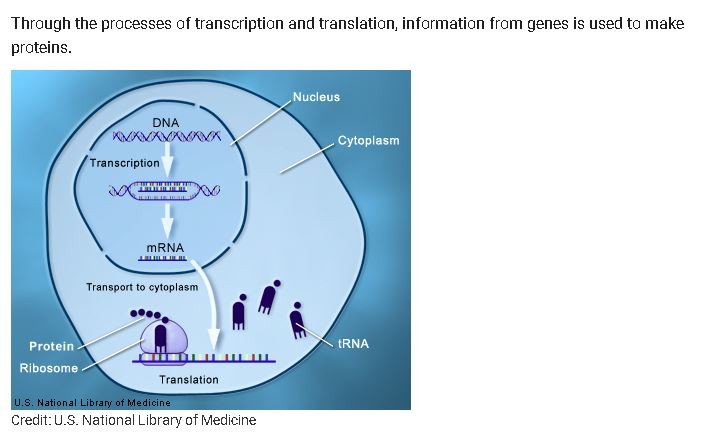
It was not quite that simple. To start with, there is reverse transcription:
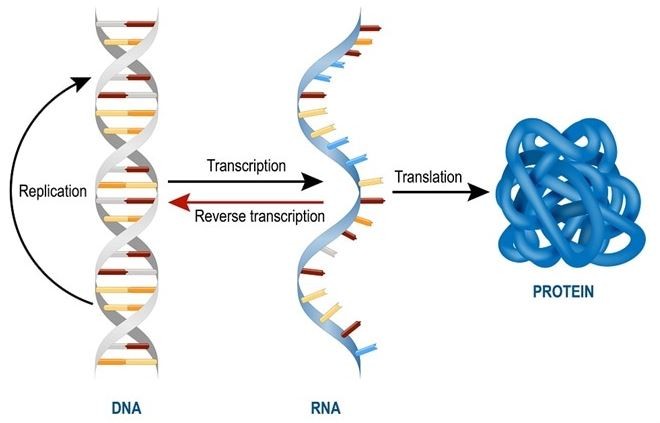
Wei-Shau & Temin 1990
Knowledge about communication in the multi-cellular organism has been going through a similar complexification. The original idea that the information source is the nervous system and the destination is a target tissue or cell has long been substituted by more complex models. Chemical communication between parts of the body, originally thought of as neuron-generated neurotransmitters and gland-generated hormones have also been substituted. First, the brain's network systems are much more complex and varied than previously thought (Preti et al 2017). Second, several other organs or tissues besides glands have an endocrine and exocrine function. With this, we now have multiple “axes” beyond the previously known hypothalamic-pituitary-adrenal, hypothalamic-pituitary-gonadal and hypothalamic-pituitary-thyroid axes.
Among the new “axes”, the one that matters to us here is the muscle-brain-adipose/liver/gut axis.
The muscle, which comprises about 40% of the weight of a non-obese individual, has long been acknowledged as being capable of altering or influencing other body functions. In the 1990s, researchers called the hypothetical substance secreted by the muscle to effectively affect other organs the “work factor” or the “exercise factor” (Pedersen 2003). Since then, myokines were identified concerning several external and internal targets.
Pedersen & Febbraio 2012
Cell signaling can be classified according to the relation between the origin and the target, and the means of transmission:
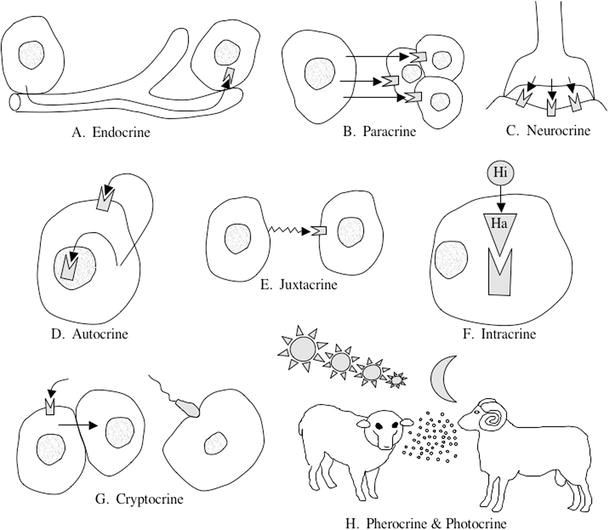
Chedrese 2009.
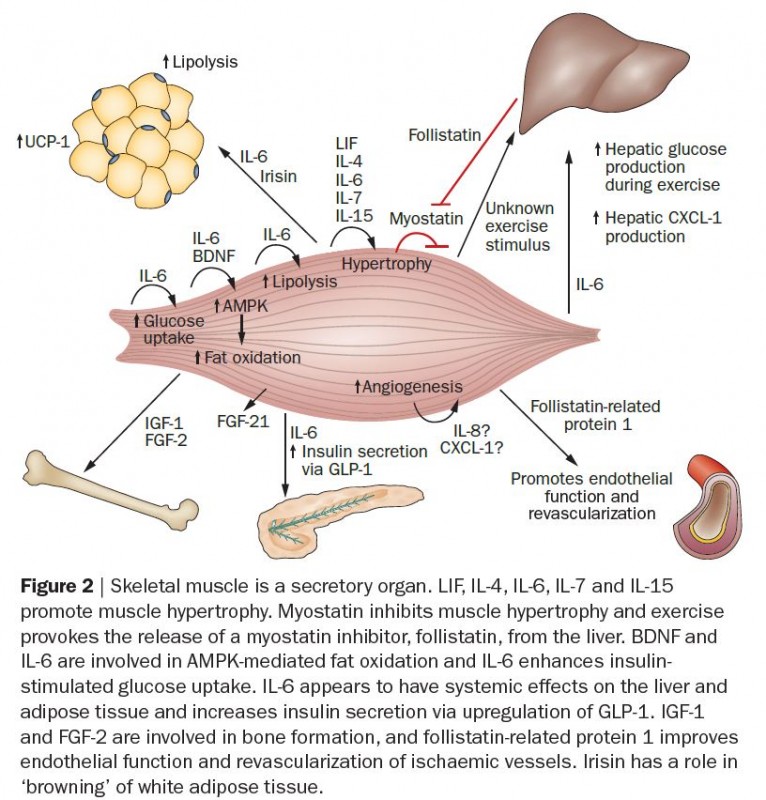
Skeletal muscle can control the type and amount of protein synthesis in response to regular exercise as well as metabolic responses in other organs. It can affect glycogen content, enhance β‑oxidation, increase sensitivity of adipose tissue to epinephrine stimulated lipolysis, and increase oxidation of intramuscular triglycerides. The most accepted hypothesis is that IL-6 (interleukin 6) is responsible for the anti-inflammatory and immunoregulatory effects of exercise.
Paillard et al 2015
The skeletal muscle can only manifest its endocrine, autocrine and paracrine actions if under constant contraction. In other words, if the individual exercises regularly. The trained muscle exhibits a different secretory profile than the untrained one (Pedersen & Febbraio 2012).
The disused muscle has a different and in some ways opposite behavior. The inactive muscle has an altered or impaired myokine response which may explain the association between sedentarism and the higher risk of many non-transmissible diseases.
Think of it as a room full of people who speak different languages, and a translator. They can communicate with each other through the translator. In the body cross-talk, every organ is at the same time an interlocutor and a translator. If you take a translator from the room, communication will be severely impaired.
Pedersen & Febbraio 2012
Inactivity: a major cause of non-transmissible and degenerative diseases
In 2004, the World Health Organization adopted the Global strategy on diet, physical activity and health in its 57th Assembly, approving resolution WHA57.17 (WHO 2004). The road to that resolution includes the acknowledgment by WHO member countries’ public health agencies of the burden that inactivity and poor nutrition represented.
Since then, more evidence accumulated supporting the increasing risks and burden of inactivity for individuals, families, and countries. More diseases were shown to be associated with inactivity and at this point, inactivity is considered a disorder (Huffman et al 2017, González et al 2017).
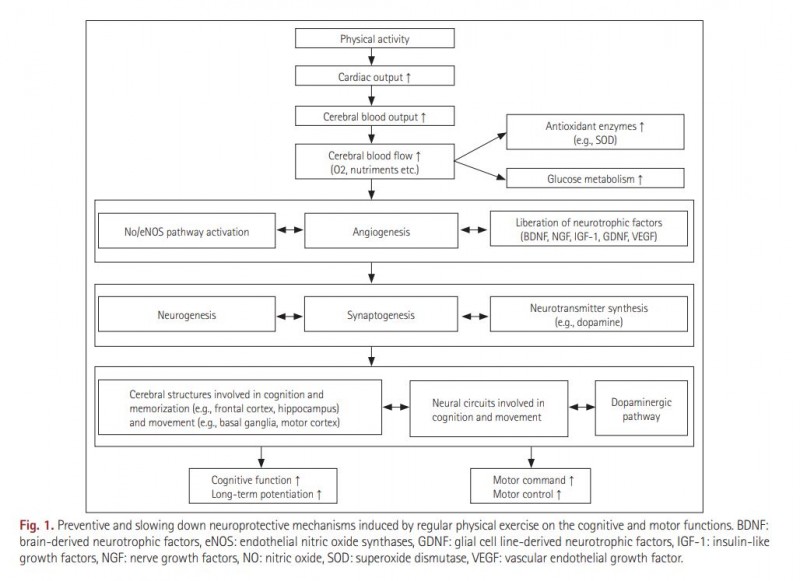
The older the individual, the higher the risk. Inactivity is associated with age-related sarcopenia (Derbré et al 2014), depression (Mamplekou et al 2010), Parkinson’s and Alzheimer’s disease (Paillard 2015), and significant losses in quality of life among cancer survivors and rheumatoid arthritis elderly patients.
Squatting from womb to tomb
The major causes of morbidity and mortality in modern urban life are non-transmissible diseases. The major burden is observed among the poor. The lower the income, the less access to healthy eating and the higher the incidence of inactivity and poor-nutrition related diseases (Drewnowski 2004). Acculturation of traditional societies also leads to losses in quality of life (Wirsing et al 1985).
Work and educational environments where individuals are seated on chairs most of the time eventually lead to losses in one of the most basic human movements: triple flexion and extension of the hips, knees, and ankles, also known as squatting.
In modern industrial urban societies, poor locomotion and loss of walking ability are common among the elderly. With a lifetime of seating on chairs, the result is the disuse of the primary muscles responsible for squatting. What follows is the vicious cycle of disuse and decay: sarcopenia (loss of muscle mass), osteopenia (loss of bone mass), degenerative diseases, depression, social isolation, even less physical activity until we end up with bedridden, sick and abandoned old people in nursing homes.
What does it mean to keep strong and conditioned until the end?
There is a consensus concerning increased inactivity among the elderly (Souza et al 2015). Time is not a constraint given that many are retired or not formally employed any longer. The factors determining increased physical inactivity among the elderly are similar to its causes: poor health, social isolation, depression, lack of information and pain (Rosqvist et al 2009). Social factors such as poverty, housing, ethnicity, and sex may also be determinant (Kaur et al 2015).
It is a vicious cycle that leads to a tragic social scenario: the elderly are condemned to slow decay and increasing levels of suffering. As technology and medical advances push longevity farther, the number of people for whom aging equals accumulated loss in quality of life increases.
This vicious cycle is not inevitable. Today, it is possible to prevent many degenerative conditions by keeping active, strong and conditioned. We must be realistic, though: it is much harder to keep active, strong and conditioned in old age. To make it worse, for the elderly, losing quality of life is much faster during periods of inactivity than for the young. Up to middle adulthood, inactive individuals may enjoy reasonable health even with bad physical activity and nutrition habits, drinking and smoking. One day, suddenly, the jolly bohemian lad or gal wakes up sick and old. What happened? Non-linearity happened. He or she was already experiencing health decline. They just didn’t notice.
If you think you are immune to all this because you are an athletic adult, think again: your chances of getting sucked in by the vicious cycle of inactivity and degenerative disorders are not so different from those of Roger, your best friend from college who never got to know where the weight room or tracks were. He was sedentary and fond of his booze. You were a college athlete and you remained as active as possible. At 50, you were skipping gym days and at 60 you didn’t bother to renew your membership. Early morning walks around the block with your canine friend were enough.
Roger and you share a room at the nursing home now, slowly drifting into the oblivion of senility, wishing you had more pain killers.
There is only one way out of this: to remain active, strong and conditioned until the bitter or sweet end.
How can we increase the likelihood of the active, strong and conditioned road as opposed to sedentarism? This is a matter of important public policy measures. The first one, however, is education. The more we spread the evidence to wider segments of society, the more we will help people in choosing healthy aging.
That is what we are doing here.
References
- Chedrese, Pedro J. "Introduction to the molecular organization of the endocrine/reproductive system." In Reproductive Endocrinology, pp. 3-11. Springer, Boston, MA, 2009.
- Cover, Thomas M., and Joy A. Thomas. Elements of information theory. John Wiley & Sons, 2012.
- Del Giudice, Marco, and Steven W. Gangestad. "Rethinking IL-6 and CRP: Why they are more than inflammatory biomarkers, and why it matters." Brain, behavior, and immunity 70 (2018): 61-75.
- Derbré, Frédéric, Arlette Gratas-Delamarche, Mari Carmen Gómez-Cabrera, and José Viña. "Inactivity-induced oxidative stress: a central role in age-related sarcopenia?." European journal of sport science 14, no. sup1 (2014): S98-S108.
- Drewnowski, Adam, and Stephen E. Specter. "Poverty and obesity: the role of energy density and energy costs." The American journal of clinical nutrition 79, no. 1 (2004): 6-16.
- El-Hani, Charbel Niño, João Queiroz, and Claus Emmeche. "A semiotic analysis of the genetic information system." Semiotica 2006, no. 160 (2006): 1-68.
- Evans, William J. "Skeletal muscle loss: cachexia, sarcopenia, and inactivity." The American journal of clinical nutrition 91, no. 4 (2010): 1123S-1127S.
- González, Karimé, Jorge Fuentes, and José Luis Márquez. "Physical inactivity, sedentary behavior and chronic diseases." Korean Journal of family medicine 38, no. 3 (2017): 111.
- Hu, Wei-Shau, and Howard M. Temin. "Retroviral recombination and reverse transcription." Science 250, no. 4985 (1990): 1227-1233.
- Huffman, Kim M., Ryan Jessee, Brian Andonian, Brittany N. Davis, Rachel Narowski, Janet L. Huebner, Virginia B. Kraus et al. "Molecular alterations in skeletal muscle in rheumatoid arthritis are related to disease activity, physical inactivity, and disability." Arthritis research & therapy 19, no. 1 (2017): 12.
- Kaur, Jasvindar, Gurpreet Kaur, Bee Kiau Ho, Weng Keong Yao, Mohmad Salleh, and Kuang Hock Lim. "Predictors of physical inactivity among elderly Malaysians: recommendations for policy planning." Asia Pacific Journal of Public Health 27, no. 3 (2015): 314-322.
- Lodish, Harvey, Arnold Berk, S. Lawrence Zipursky, Paul Matsudaira, David Baltimore, and James Darnell. "Molecular cell biology 4th edition." National Center for Biotechnology Information, Bookshelf (2000).
- Mamplekou, E., V. Bountziouka, T. Psaltopoulou, A. Zeimbekis, N. Tsakoundakis, N. Papaerakleous, E. Gotsis et al. "Urban environment, physical inactivity and unhealthy dietary habits correlate to depression among elderly living in eastern Mediterranean islands: the MEDIS (MEDiterranean ISlands Elderly) study." The journal of nutrition, health & aging 14, no. 6 (2010): 449-455.
- Paillard, Thierry, Yves Rolland, and Philipe de Souto Barreto. "Protective effects of physical exercise in Alzheimer's disease and Parkinson's disease: a narrative review." Journal of clinical neurology 11, no. 3 (2015): 212-219.
- Pedersen, B. K., A. Steensberg, C. Fischer, C. Keller, P. Keller, P. Plomgaard, M. Febbraio, and B. Saltin. "Searching for the exercise factor: is IL-6 a candidate?." Journal of Muscle Research & Cell Motility 24, no. 2-3 (2003): 113.
- Pedersen, Bente K., and Mark A. Febbraio. "Muscles, exercise and obesity: skeletal muscle as a secretory organ." Nature Reviews Endocrinology 8, no. 8 (2012): 457.
- Preti, Maria Giulia, Thomas AW Bolton, and Dimitri Van De Ville. "The dynamic functional connectome: State-of-the-art and perspectives." Neuroimage 160 (2017): 41-54.
- Rosqvist, E., E. Heikkinen, T‐M. Lyyra, M. Hirvensalo, M. Kallinen, R. Leinonen, M. Rasinaho, I. Pakkala, and T. Rantanen. "Factors affecting the increased risk of physical inactivity among older people with depressive symptoms." Scandinavian Journal of Medicine & Science in Sports 19, no. 3 (2009): 398-405.
- Shannon, Claude E., and Warren Weaver. The mathematical theory of communication. University of Illinois press, 1998.
- Shannon, Claude Elwood. "A mathematical theory of communication." Bell system technical journal 27, no. 3 (1948): 379-423.
- Souza, Adelle MR, Gerda G. Fillenbaum, and Sergio L. Blay. "Prevalence and correlates of physical inactivity among older adults in Rio Grande do Sul, Brazil." Plos one 10, no. 2 (2015): e0117060.
- Wirsing, Rolf L., Michael H. Logan, Marc S. Micozzi, David Ondieki Nyamwaya, Tola Olu Pearce, Domeena C. Renshaw, and Otto Schaefer. "The health of traditional societies and the effects of acculturation [and comments and replies]." Current Anthropology 26, no. 3 (1985): 303-322.
- World Health Organization. "Global strategy on diet, physical activity and health. Geneve: World Health Organization; 2004."
- Ye, Jessica, and Ruslan Medzhitov. "Control strategies in systemic metabolism." Nature Metabolism 1, no. 10 (2019): 947-957.

At 61 and running into some hip issues with squatting, I’m trying to find new ways to program my training. Not a lot of information.
Maintenance of 1. Strength ,2. Cardiovascular fitness. 3. Body mass proportion ( not BMI, but say a waist to chest or shoulders ratio, %bf etc...). 4. Mobility.
Incorporating those aspects with a recoverable program for the over >55 crowd would be a great read.
Thank you for the article, very thoughtful.
1) Lee, I'll focus on that. It's a big challenge and I'll try to reach into the literature of both frequent issues among us >55 crowd and how to address them while and into a training program and specificities of the items you mentioned. The young folks won't like it :) haha. Well, on the down side, if you don't die young, you age. On the flip side, too, if you don't die young, you age!
2) Evan, yes, eventually it will have to come to something like a program. I'm really not a fan of detailed, one-way strategies (conventional programs) because they end up frustrating those dealing with individual issues. I'm in favor of of programs that help people like an algorithm: "if A, then B. If not A, then C" and so on.
Thank you very much!