










In part one of this series, we discussed the topic of tissue load versus tissue capacity and how it relates to injury prevention and injury rehabilitation. If you have not yet read part one, I recommend reading it to understand the starting point of this article. To briefly summarize, tissue load refers to any internal or external load that is placed upon a muscle tissue and its supporting structures. These supporting structures include ligaments, tendons, cartilage, and fascia. Tissue capacity refers to the muscle tissue and the capacity of its structures to absorb load without injury. This varies between types of tissues, as well as the activity.
This second article of the series will discuss additional loading concepts, training considerations, and rehabilitation protocols for increasing tissue capacity while maintaining or decreasing training load. This information is educational material aimed towards the rehabilitation of musculoskeletal and soft tissue injuries but is not meant to treat or diagnose an injury. Please seek a medical professional if you are injured.
RECENT: Tissue Load vs. Tissue Capacity: A Key to Injury Recovery and Prevention
Common practice in traditional rehab settings is to reduce direct load to the target tissues. This, by no means, is incorrect. By doing this you also reduce load to the surrounding supporting tissues. When the traditional rehab phase begins, standardized loading increases to the target tissues but not directly to the surrounding tissues. So, while the main injured area is resting (by reducing training load) the tissue capacity of the surrounding muscles is also being decreased via a decreased general training load. Alas, when the injured tissues get stronger without loading the surrounding tissues, another injury occurs. This is how subsequent injuries continue without the same exact injury occurring multiple times.
Increase the tissue capacity of the surrounding muscles as well as the injured tissues for optimal results.

A Different Approach to Looking at Things
When looking at the state of an injury, whether in a clinical setting or gym setting, there are a few things that must be taken into consideration before starting to increase tissue capacity:
- What demands are being asked of the tissues and what is the current state of capacity of those tissues?
- What is the current training age?
- What is the movement age?
- Do they have the prerequisite movement competency to perform the exercise(s) of activity or is this something completely new to them?
- Are they lacking the physical fitness needs of the sport or activity (i.e., endurance, strength, power, flexibility, mobility, stability, balance)?
- What are the tissue capacity demands of the sport or activity?
- Is there a large amount of energy transfer necessary?
- Is there a reliance on eccentric or concentric control?
- Is there a need for controlled landing, or the stretch shortening cycle?
Once you have established the above and have taken an inventory of your tissue demands versus your current tissue state, you can put together a needs list and begin to structure your rehab. The process goes from strength, to energy storage, and to energy release.
Strength
This refers to they type of muscle action you will use to begin increasing the tissues' abilities to contract. The only way a muscle can increase its true tissue capacity is to build its volume of contractions without going above the tissue demands. I use a dose response continuum to quantify this. The goal is to find the optimal load and type, and build volume slowly over a period of low frequency to high frequency.
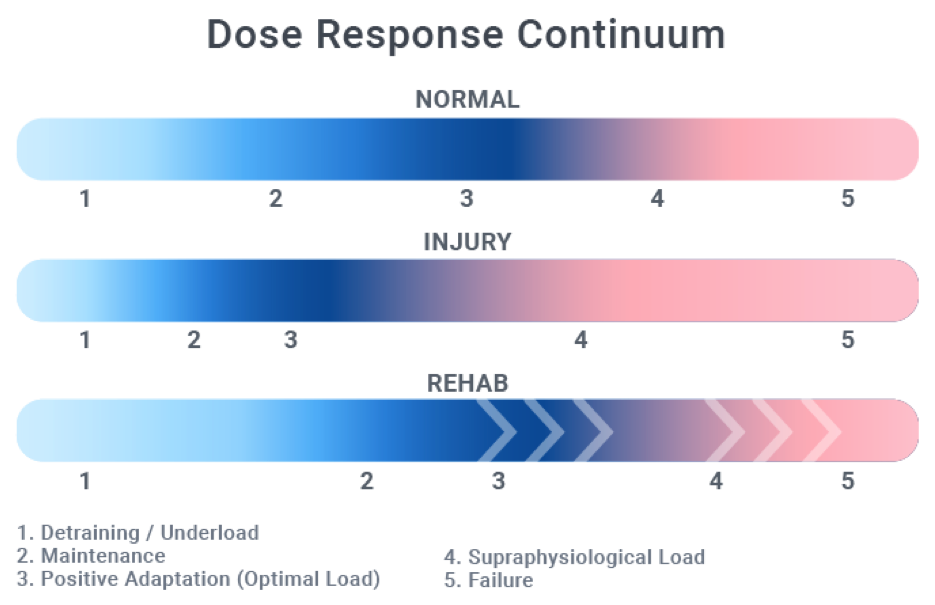
As you can see from the image above, there are two sides to the continuum — the right being the side that will cause adaptation. If you go too far right you will impose tissue damage because you are above the tissue capacity threshold. On the far left, you have the area in which the load is not great enough to place change. This can also be too low where the muscle regresses.
Our goal is to drive the continuum to the right. This will leave less room for injury because we increase the range in which we can maintain or even create a positive adaptation. However, this also means it leaves the gap for supra-physiological adaptations to be smaller. However, in my opinion, this means the gains will be truer! Optimal contractions include isotonic, isometric, concentric-only, and slow concentric movements. These place larger demands on the muscle tissue without adding too much load to the tendon or ligament. Because most injuries occur at the musculotendinous junction, these are “more” optimal.
Energy Storage
This refers to the type of energy that will be transferred in the muscle contraction. For example, is this an explosive lift that requires a high transfer of energy, or is this a slower energy transfer like one found in aerobic activities such as running. Identifying this will help you take the newly strengthened muscle and begin to convert it closer to its sport or activity demands. To further illustrate, let's look at a powerlifter. The energy transfer demands are high and explosive. This means higher demands placed on tendons and ligaments. It is best to use up to 70% of maximum voluntary contraction when building tissue capacity. We can then use training tools such as over-eccentrics to build the tendon-muscle connection and increase our tissue capacity further. For sports such as soccer, baseball, basketball, etc., that involve a higher demand in change of direction and speed, we can begin to add in slow directional changes in movement to further specify our rehab. This is why you must combine function and load.
Energy Storage Release
We now start to become more specific in our demands of releasing the energy stored in our tissues. We have been increasing our tissue capacity by placing optimal loads (a maximum of 70%) using correct contraction types, while building frequency. It is now time to slowly move to a higher dynamic correspondence by mimicking or practicing the sport or activity. Moving to sport-specific activity, functional movements, and energy system training are all part of this phase. Getting to and rehabbing in this phase can take up to 12 weeks. This is dependent on many internal and external factors.
Interventions
These refer to the things we can do to help decrease the tissue load and or contributing factors to the increased tissue load. The following are just examples.
Stressors:
- Decrease movements that elicit pain
- Decrease training frequency
- Modify position or posture
- Decrease repetitive movements
- Increasing general patient knowledge
- Manual therapy (when appropriate)
- Shift dose response continuum to the left (leaves more room for adaptation)
Actions:
This is the meat and potatoes of increasing tissue capacity.
- Progressive overload
- Training continuum guidelines
- Decrease neural sensitivity (nociception)
- Decrease movement fear
- Increase movement patterning
- Increase movement efficiency and quality
Programming Considerations
We need to remember that our tissue adaptations are only as good as the loads we place on them. The higher the loads, the greater the demands of our tissues to increase its capacity (to a point). This is why heavy loads are essential, but optimal heavy training loads are king.
Most training injuries will occur after times where tissues are coming off long rest periods and when tissue capacity has time to decrease. This can happen as quickly as 14 days. This might be time off from an injury, deloads, or simply taking a vacation. It is important to return slowly, regardless of the amount of time off, and build tissue capacity back to its normal levels before seeking supraphysiological adaptations.
Build frequency first then volume per training session. Stay at 70% of maximum voluntary contractions. Pain is not an indication of needing to stop. You can have pain and not be causing any further harm. Monitor this for feedback.
Athlete Considerations
Pre-Season: In terms of building tissue capacity, aim for increasing to a higher frequency before increasing load. Slowly build load up over an increasing frequency, then pull back frequency to find your sweet spot.
In-Season: A little goes a long way. One to two sessions per training week at moderate volume below or at maintenance will suffice. This ensures tissue capacity will stay functional and not decrease. Slowly build towards the tail end of your season into your off-season. Loads should stay at or below 70%. Volume is dependent on the athlete's capabilities, playing time, training age, etc.
Off-Season: Slowly build volume and frequency to medium to high. Loads will increase above 70% but depend on training system being used.
It is important for the sports coach, strength and conditioning coach, trainer, physical therapist, athletic trainer, movement guru, etc., to understand the tissue load versus tissue capacity continuum in order to help bridge the gap from injury to performance. Hopefully, you have a good understanding and outline to help you move forward in the right direction. If you have any specific questions regarding specific injuries please feel free to email me at performanceandrecoverysystems@yahoo.com or visit www.performanceandrecoverysystems.com.
