










Femoro-acetabular impingement is a common injury affecting high-level athletes to middle-aged general populations. The mechanism of FAI can vary depending on age levels, anthropometry, and activity levels among other things. The diagnosis of FAI can be a simple procedure that doesn’t have to include magnetic resonance imaging (MRI). The diagnostic procedures were discussed in Part 1 of Femoro-Acetabular Impingement and the Rehab Process series.
Following a positive diagnosis of FAI, the rehab protocols are a debated topic among researchers and practitioners and are often not fully understood. The general rehab procedure of FAI involves glute activation, single leg stability work, gait critiquing, and hip capsule mobility work, all of which are of the utmost importance in the rehab procedure.
RECENT: Femoro-Acetabular Impingement and the Rehab Process: The Diagnosis
Research was performed in 2010 (4) in regards to soft tissue therapy and the recovery/rehab of FAI. The areas of concern were the hip abductors, external rotators, and the TFL. The study showed reasonable results in that the subjects showed some pain relief. However, a limited area of research and a very commonly overlooked aspect of the cause of FAI and SI joint pain (as discussed in Part 1) is the Iliotibial band (IT band). The IT band can be a major player in the cause of FAI and should be an initial point of concern in the rehab procedure of FAI.
Aksana Kulchytskaya © 123rf.com
The Controversial Topic of Soft Tissue Therapy and the IT Band
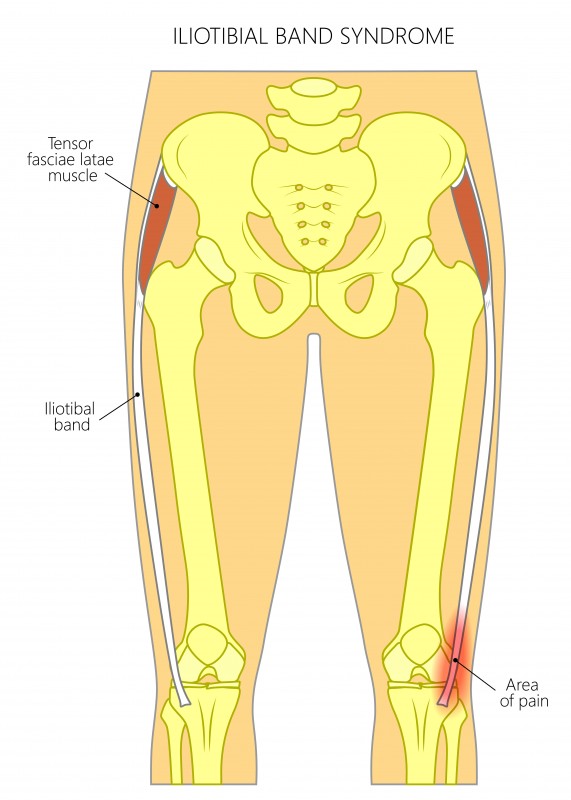
The IT band has been a controversial topic in the world of physiotherapy/strength and conditioning over the past few years. The IT band is a fibrous connective tissue, originating from the tendons of the tensor fascia latae (TFL) and the glute max and inserting into the lateral epicondyle of the tibia. As the IT band crosses the knee and hip joint, it is a bi-articular structure and does play a role at the hip joint (contributing to movement) and at the knee joint (contributing to stabilization). (2)
The primary argument in regards to the IT band and why it shouldn’t be foam rolled is that the IT band is made up of connective tissue. Connective tissue is made up of collagen, which is a far more dense substance than muscular tissue. The extreme density of collagen makes creating a change in the tissue almost impossible. The argument against foam rolling the IT band is that the IT band can’t be lengthened and that foam rolling/stretching it in any way will cause no effect to the tissue itself.
If the true effect of myofascial release (more correctly termed “self-assisted manual therapy”) was known, then this argument, based on the assumption that foam rolling causes a physical effect to the structure of the muscular tissue, would be true.
However, the true effect of foam rolling on muscular tissue is very inconclusive. Many theories have been proposed but none have even begun to scratch the surface on the true reasoning as to why it works
For a very detailed article on the different theories on the benefits of foam rolling, read Chris Beardsley and Bret Contreras' "Foam Rolling and Self-Myofascial Release."
The one conclusion that people have though, is that it does work. Kelly Starrett, with his book Becoming a Supple Leopard, has helped hundreds of thousands, and possibly millions, of people around the world without a reference in sight. As wrong as this may be, to some people and the scientific community as a whole, what is truly important is what brings results, whether it be based on scientific research or anecdotal evidence. Kelly Starret may not be as backed by research as one might like, but anecdotally, his practices have helped people, which is what really matters. (5)
The lack of conclusive evidence in regards to the structural effect of foam rolling on muscular tissue accidentally debunks the theory that the IT band shouldn’t be foam rolled. It has been shown to take over 9,000 newtons (extremely far outside potential physiological range) of force to structurally change the TFL’s muscular tissue by one percent. So if foam rolling causes no structural change in muscular tissue (but still gives a pain/tightness relieving sensation), the argument that you shouldn’t foam roll the IT band because of its tautness is redundant. (1)
The IT Band's Effect on the Sacro-Iliac Joint and Femoro-Acetabular Impingement
The IT band is most commonly referenced in regards to the IT band syndrome, which is chronic pain on the outside of the knee (the recovery of IT band syndrome is well documented and is actually very seldom caused by the IT band, but that topic is for another article). However, a lesser talked about symptom of a tight IT band is sacro-iliac (SI) joint pain and its role as a factor in femoro-acetabular impingement (FAI).
FAI is generally tested for using the FADDIR (Flexion, Adduction, Internal Rotation) Test, in which a positive test indicates FAI. The primary symptom of FAI is locking or clicking in the front of the hip/groin and is often associated with SI joint pain in the form of a dull ache in the side of the lower back, especially when bracing heavily, forward bending, lateral bending, rotating, or a combination of all four. (Symptoms and diagnoses were discussed further in Part 1 of this series.)
The research regarding surgery and FAI has shown extremely mixed results, so the initial recommended procedure for improving FAI is through a more conservative non-invasive approach. The non-invasive procedure to improving the symptoms of FAI generally consists of glute activation work, postural corrections, and gait critiquing, all of which are of the utmost importance and should be used to a good extent throughout the rehab procedure. However, a very often overlooked aspect of the rehab process (and a potential issue in the first place) is the tightness of the IT band. (6)
As discussed in Anatomy Trains by Thomas Myers, the body should truly be looked at from a global perspective, and all structures have some effect, no matter how small or large on all other structures. The IT band, the TFL, The glutes, the QL, and the external obliques are all a part of the lateral line (one of the nine meridians outlined in Anatomy Trains) and are all close structures to each other, and therefore, all affect each other in one way or another. Tightness in the belly of the IT band will often cause a chronic de-activation in the TFL and glute muscles. De-activation of the TFL and glute is associated with overcompensation of the QL/external oblique and is a very common cause of SI joint pain. (3)
De-activation of the glute is also associated with FAI and all of its symptoms. The location of the symptoms of FAI will often make people associate this pain (locking/clicking in the front of the hip) with the psoas. The psoas can be problematic in relation to FAI but should not be the primary diagnosing point. The de-activation in the glute/TFL caused by the tight IT band causes a reduction in hip external rotation range and hip extension range. A lack of range through these movements can cause much-unwanted shear strain on the labrum between the femur and pelvis, especially during high force movements such as running, squatting, landing, etc. For this reason, the tightness of the IT band can heavily contribute and will often be one of the primary factors in regards to FAI.
The loosening of the IT band should, in general, be the initial procedure performed in the rehab process of SI joint pain or FAI. A chronically tight IT band will greatly restrict the glute/TFL and its ability to perform their respective functions. As a base, IT band loosening should be performed before glute activation or postural/gait correction work to see the full benefit of said correction work.

Self-assisted manual therapy of the IT band with a barbell. Note: The foot is turned in to allow the bar to sit on the outside of the thigh.

Self-assisted manual therapy of the IT band with a foam roller.
It should be noted that due to the limited research in regards to the IT band and FAI, the mechanism of why the IT band causes hip and SI joint pain is based on the author’s experience and self-research. Although the mechanism and reasoning discussed is a very well educated hypothesis, the author is open to discussion and potential correction in regards to the physiological mechanisms as to why a tight IT band causes pain in the hip and SI joint.
Conclusion
Soft tissue therapy is an undeniably important aspect of the rehab process of FAI. The researched areas of concern have predominantly been the hip abductors, external rotators, and the TFL, which are important areas to focus on. However, an overlooked area of concern is the IT band as a causing factor of FAI.
The IT band is a taut structure of connective tissue that is almost impossible to structurally change. However, given the inconclusive research as to the effect of self-assisted manual therapy, the argument that the IT band shouldn’t be foam rolled due its tautness is redundant.
Anecdotally, the foam rolling of muscular tissue has shown to be an extremely effective procedure in the prevention and reduction of symptoms within a number of injuries and has also shown to be effective in the improvements of mobility and flexibility when performed correctly and consistently enough.
The IT band is no different than muscular tissue in how the “loosening” of said tissue is of great benefit to the athlete and general population as a whole. The “loosening” of the IT band should be seen as an initial stage of the procedure in the rehab of SI joint pain and FAI, as the full benefit of glute activation/postural correction work cannot be seen if a chronically tight IT band is constantly pulling and causing activation problems within the glute/TFL.
References
- Findley, Thomas, et al. "Fascia research–a narrative review." Journal of bodywork and movement therapies 16.1 (2012): 67-75.
- Flato, R., Passanante, G.J., Skalski, M.R., Patel, D.B., White, E.A. and Matcuk, G.R., 2017. The iliotibial tract: imaging, anatomy, injuries, and other pathology. Skeletal radiology, 46(5), pp.605-622.
- Myers, T.W., 2013. Anatomy Trains E-Book: Myofascial Meridians for Manual and Movement Therapists. Elsevier Health Sciences.
- Cashman, G.E., Mortenson, W.B. and Gilbart, M.K., 2014. Myofascial treatment for patients with acetabular labral tears: a single-subject research design study. journal of orthopaedic & sports physical therapy, 44(8), pp.604-614.
- Starrett, K. and Cordoza, G., 2013. Becoming a supple leopard. The ultimate guide to resolving pain, preventing injury, and optimizing athletic performance.
- Wahoff, M. and Ryan, M., 2011. Rehabilitation after hip femoroacetabular impingement arthroscopy. Clinics in sports medicine, 30(2), pp.463-482.
Noel FitzGibbon is a former international underage-level weightlifter who has represented Ireland at the European level and has achieved a World Ranking with the IWF. He has coached in strength and conditioning and weightlifting/powerlifting at a provincial, national and international level. He is currently working as a personal trainer and a strength and conditioning coach out of Calgary, Canada.
Part 1: The Diagnosis
