








Every year, it’s the same trend: lose weight and lose fat. Although weight loss and fat loss are used interchangeably, they differ in their long-term effect, and elicit different training and lifestyle implications. The last few years has seen the birth of consuming more fats; mono, and poly-unsaturated fatty acids, and the ever-so evil (so we think) saturated fats. Despite the high-powered celebrity endorsements, dubious testimonials, books, and media outlets and notwithstanding more scientific evidence contradicting the original medical advice about “fats”, we continue to be (unfortunately) a society that is undoubtedly swimming in dogma.
What is dietary fat? How does it work? Do we get fat by eating fat? This “anti-fat” movement has actually created more problems than solutions. Do we really increase body composition by consuming fats? Let’s talk about it. Bust out your muscle cars and nitrous oxide systems, welcome to “The Fat and the Furious.”

A Brief History
We’ve all heard and witnessed the never-ending cycle about the war on carbs. Well, we can certainly liken this to the “war on fats”. Dietary fat has been demonized for years, dating back to the 1970s when the low-fat diet was recommended to all Americans. Scientists had evidence that foods with saturated fat such as eggs and meat could increase LDL cholesterol. However, there were a lot of complexities that scientists didn't yet understand, and certainly not a lot of data at that time. Our disdain of saturated fat originated from the 1950s, led by the infamous Ancel Benjamin Keys, a scientist who relentlessly championed the idea that saturated fats increased cholesterol levels and, as a result, caused heart attacks. His original body of research [1] led us to believe saturated fat was the main culprit involved with heart disease. Despite the fact there existed numerous flaws in his data, it erroneously convinced everyone that dietary fat was indeed evil. It was known as the "Seven Countries" study that he conducted on nearly 13,000 men in the U.S., Japan and Europe allegedly demonstrated that heart disease wasn't the inevitable result of aging but could be associated with poor nutrition [2]. It was learned that Keys violated several basic scientific principles in his research. For example, instead of choosing countries randomly, he selected only those likely to prove his own beliefs. This idea began its prolific journey during this time as Americans faced a fast-growing epidemic in heart disease. In fact, the president during this era, President Dwight D. Eisenhower suffered a heart attack in 1955. Therefore government agencies were on the prowl. Although a deep a history does exist, in the early 1960’s, Key’s sealed the deal on the evil-eyed saturated fats by accepting a position on the nutrition committee of the American Heart Association. Despite the fact the committee had originally been highly skeptical of his theory, it issued, in that same year, the country's first-ever guidelines pointing towards saturated fats.
Beginning in the late 1980s, major reports surfaced identifying dietary fat as the number one target and dietary change needed to improve various markers of health. Hence, some of the fat was indeed saturated. Although the intentions were genuine (at the time), the idea was to reduce saturated fat. However, the assumption was that it was too complicated and that if people simply decreased their fat intake, their lifestyle and other dietary markers would also improve. Unfortunately, this message was lost in translation, and to the dismay of many American’s and science experts, the food industry would substitute vegetable fats for animal fats in such a profound and drastic manner, and would also substitute sugars for fats, whiling keep the calorie content exactly the same. By these new standards (or should we say unscrupulous methods), the creation of the “low fat” mythology began, whereby falsely blaming low fat for the obesity crisis. Before we move forward, and before you may become “furious” (pun intended), it’s important to discuss the fundamental nature of fats, their role in physiology and nutrition.

Fat Files 101
For numerous reasons, many continue to believe fat is a messy, physiology tissue nesting in your body, invading the aisles at your local grocery chain, debilitating every physiological system, and responsible for numerous diseases and disabilities. True, too much body composition is a risk factor for disease but that’s not the point here. The point is that fat is good, especially the right types.
Fat serves numerous important functions, as it provides a crucial and strategic role for the structure and flexibility of cell membranes, regulating substance movement through those membranes. It’s no secret that the most well known function of fat is as an energy reserve. Fat yields more than two times the calories per gram than that of carbohydrate and protein (9 calories/gram for fat vs. 4 Calories/gram for carbohydrate and protein). It has been estimated that lean adult men store about 131,000 calories in fat [3]; enough energy to sustain life for the average person for approximately 65 days. Fat is stored in the body in the form of triglycerides. Triglycerides are made up of three fatty acid molecules and a molecule of glycerol. The mobilization of fat refers to the initial process of releasing fat from storage sites (adipocytes) in adipose (fat) tissue. Lipolysis (or fat breakdown) is the sequence of reactions that biologically 'strip' the triglyceride into three fatty acids and glycerol, which are released into the blood [4]. The metabolism of fat describes the complete biological breakdown or oxidation of fatty acids into energy that can be used by the cells of the body. Fats also assists in carrying fat-soluble vitamins (A, D, E and K) throughout the body in efforts to perform important functions. It helps regulate the taste of food, aids in cooking (even cooking oils) and has profound effect on satiation [5]. Further, distinct types of fat (known as eicosanoids, derived from Omega 3 and Omega 6 fatty acids) are involved in specialized hormone signaling, exerting intricate control over many bodily systems, mostly in inflammation or for immune function [5, 6]. Fatty acids also regulate gene expression, controlling the types of proteins cells generate, and alterations in gene expression affect metabolism, inflammation, and cell growth and division.
It’s important to discuss the specific types of fat, as fat is often categorized as “evil” across the board regardless of what type. Fat is often disparaged as a cause for everything from weight gain, to cholesterol to decreasing your max effort squat. In turn, this creates a misleading agenda making many people believe they need to avoid fat at all costs. Fat can be categorized into several classes; saturated fats, unsaturated fats, and trans fats, with varying types in each class. One of the most misunderstood characteristics of dietary fat (similar to calories) is the perception that all fats are created equal. They are not.

Let’s start with some basic terminology:
The Fats of Life
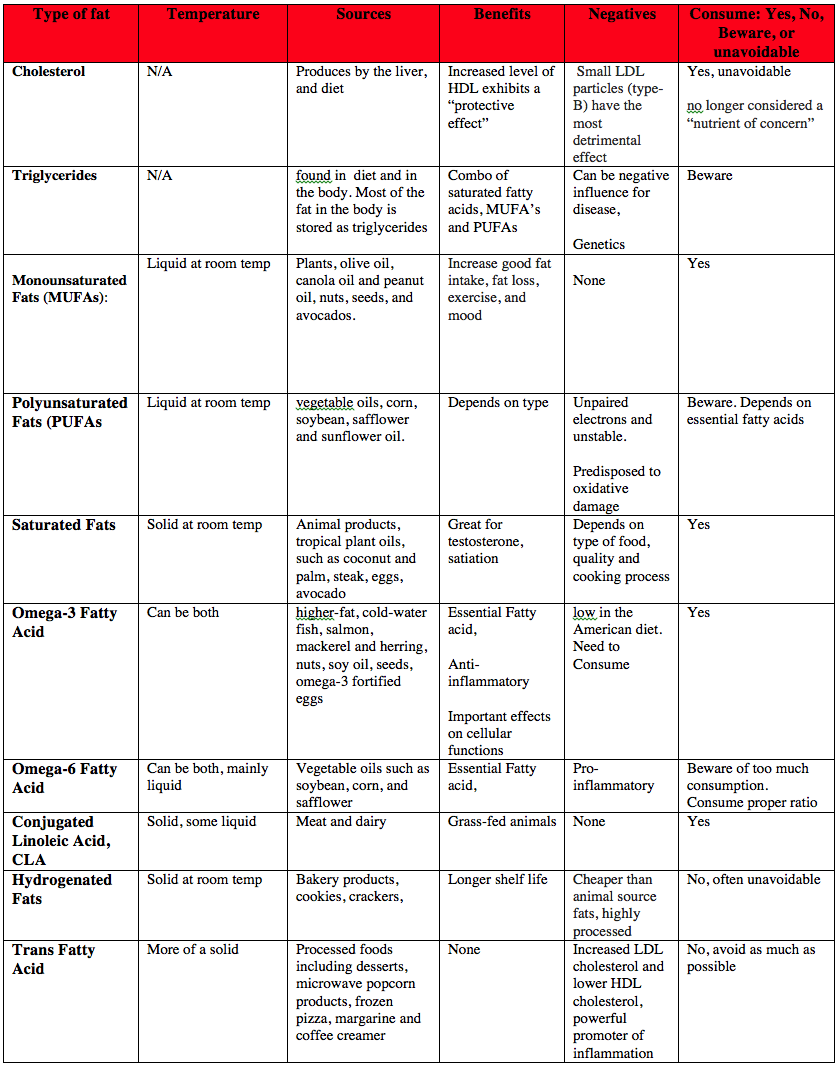
Cholesterol
Cholesterol is a waxy substance, found in animals and people. Technically a sterol, (which is a combination of a steroid and alcohol), cholesterol is an important constituent of cell membranes. The vast majority of cholesterol in the body is produced in the liver, while the rest is absorbed from the diet. A special form of cholesterol in the skin (cholecalciferol) has the ability to change into vitamin D when exposed to sunlight; sex hormones, and bile acids needed for digestion [7-9]. There are two different types of cholesterol: 1). Blood, or serum cholesterol, which circulates in the blood and is mostly produced by the body, and 2). Dietary cholesterol derived from food or animal origin. The theory that fat and cholesterol cause heart disease became widely accepted despite much evidence to the contrary.
Cholesterol is transported in the blood by different carrier protein called lipoproteins.Four main classes of lipoproteins have been categorized: chylomicrons, (from the intestinal absorption of triglycerides), very low density lipoprotein (VLDL), made in the liver for the transport of triglycerides; low-density lipoprotein (LDL), a product of VLDL metabolism and the primary transporters of cholesterol; and high-density lipoprotein (HDL [5]. The two major blood cholesterol carriers are LDL, and HDL. HDL is the smallest of the lipoprotein particles and enables the transportation of triglycerides through the bloodstream [5]. It also utilizes and excretes LDL from the body by delivering it to the liver, as it acts as scavenger, which is why HDL is referred to as the "good" cholesterol. An increased level of HDL exhibits a “protective effect” against cardiovascular disease, as lower levels of HDL raise your risk of heart disease. With an increase level of HDL (60 mg/dl or higher), one can knock off a negative risk factor. Although complicated, it is actually a combination of two primary types: the large, fluffy pattern A (think of these as an average medicine ball), and the small, dense pattern B (think of these a the size of popcorn seeds). Most people are not aware that it’s the particle size that makes all the difference, as small dense LDL particles (type-B) are the most detrimental effect as they are more likely to lodge themselves in arterial walls. However, it’s possible to have normal or even low cholesterol level, but a high number of LDL particles [10]. An increased level of HDL exhibits a “protective effect” against cardiovascular disease, as lower levels of HDL raise your risk of heart disease. With an increase level of HDL (60 mg/dl or higher), one can knock off a negative risk factor. However, recent studies refute the belief that raising HDL will uniformly change into reduced rate of heart disease across the board, as genetics are often an influence [11].
Our bodies have the ability to make all of the cholesterol needed for proper functioning, but most people also get it from foods. The theory that fat and cholesterol cause heart disease became widely accepted despite much evidence to the contrary. Fact is, in the month of February, numerous media reports have surfaced and many of the nations top nutrition advisory panels have decided to drop its caution about eating cholesterol-laden food finding that cholesterol in the diet is no longer considered a “nutrient of concern.” Hell, it only took 40 years.

Triglycerides
Scientific name for the main form of fat found in the diet and in the body. As previously mentioned, most of the fat in the body is stored as triglycerides (TAGS) which are made of three fatty acids, and molecule of glycerol. It’s within these fatty acids can include any combination of saturated fatty acids, monounsaturated fatty acids (MUFAs), and polyunsaturated fatty acids (PUFAs).
Monounsaturated Fats (MUFAs)
These fats are liquid at room temperature (containing less hydrogen atoms). A biochemical difference between these fats is that they are missing one pair of hydrogen atoms. Monounsaturated fats are primarily from plants and include olive oil, canola oil and peanut oil, nuts, seeds, and avocados. A major cornerstone of MUFAs lies in the vaunted in Mediterranean diet, which has been suggested for years for improving numerous health markers. [12-14]. Those individuals wanting fat loss and to increase good fat intake, MUFAs are a great and appealing strategy. Further, a 2013 study in The American Journal of Clinical Nutrition reported that substituting dietary monounsaturated fat for saturated fat is associated with increased daily physical activity and resting energy expenditure and with positive changes in mood [15].
Polyunsaturated Fats (PUFAs)
Similar to MUFA, PUFAs are also liquid at room temperature. Examples include common vegetable oils, such as corn, soybean, safflower and sunflower oil. However, they are missing two or more unsaturated double bonds in their carbon chain. Meaning, PUFAs can be unstable, as they possess unpaired electrons, which makes them highly susceptible to heat and oxygen. When exposed, these highly unstable fats oxidize making them predisposed to oxidative damage in the body. PUFA’s can often be a real Jekyll and Hyde, as they include the essential fatty acids, omega 3s, but also omega-6 (see below for more info).

Saturated Fats
Here is it, the almighty villain, or is it? Until the last few years, saturated fat was at the top of America’s Most Wanted list, but thankfully society and research has changed their views on saturated fat, although it does continue to be chastised. Usually solid at room temperature, saturated fats have all of the hydrogen atoms they can grasp (saturated with hydrogen). These fats are primarily from animal products, but are also found in tropical plant oils, such as coconut and palm. A fundamental difference between saturated and PUFAs are that saturated fats are more stable due to the fact they have no unpaired electrons. In addition, it’s a huge player in the production of sex hormones, such as testosterone. Many strength athletes can benefit from saturated fats intakes (i.e. steak and eggs, avocado). A study published in the American Journal of Clinical Nutrition [16] randomly assigned 45 men to either a high fat/low fiber or a low fat/high fiber diet. The subjects followed each diet for ten weeks. The high fat/low fiber diet periods yielded 13% higher levels of total serum Testosterone compared to the low fat/high fiber diet period. Another study from the International Journal of Sports Medicine [17]enrolled eight strength athletes and ten active non-athletes. After comparing the subject's dietary analyses and blood tests, it was shown that only the strength-training athletes had significant correlations between fat intake and Testosterone levels. Porterhouse steak, anyone?
Omega-3 Fatty Acid
A main essential highly polyunsaturated fatty acids are Omega-3s. The three main omega-3 fatty acids are: alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Omega-3 fatty acids are largely found in higher-fat, cold-water fish, such as salmon, mackerel and herring, nuts, soy oil, seeds, as well as omega-3 fortified eggs [5]. EPA, and DHA are known as the “long-chain” omega-3 fatty acids since they are mainly found in fish and fish oils. EPA and DHA have the most potent health benefits of the omega-3 fatty acids. However, they are particularly low in the American diet, and since conversion of ALA to EPA and DHA is poor, thus needing intake by everyone. Diets high in omega-3 fatty acids (particularly fish oils) have been researched for years in improving numerous markers of health and disease, acting a both an anti-inflammatory and improved brain function, reduced cancer risks and improved moods, and have have several important biological effects on a range of cellular functions [18, 19].

Omega-6 Fatty Acid
Known as linoleic acid, these types of fats are considered essential, and can be found in vegetable oils such as soybean, corn, and safflower. Omega-6 fatty acids are also found in many baked goods and some fried foods and nearly ubiquitous in restaurants. But, herein lies the rub. The main concern for this type of fat is pure overconsumption. So why the mere onslaught? Well, these fats are myriad with pro-inflammatory properties (Omega-6 is pro-inflammatory, while omega-3 is anti inflammatory) [20] due to the fact these fats contain a higher percentage of omega-6 vs. omega-3, as omega-6 and omega-3 fatty acids compete for the same conversion enzymes. To keep things simply, the more omega-3 fat you consume, the less omega-6 will be available to the tissues to produce inflammation. In essence, it’s all about the proper ratio. People who consume a non-industrial diet have an Omega-6:Omega-3 ratio of about 4:1 to 1:4, or somewhere in between. Unfortunately, the ratio is today’s era is nearly is 16:1 [21]. Damn Gina!
Conjugated Linoleic Acid, CLA
This fat has gain enormous popularity in recent years. The double bonds of CLAs are conjugated (polyunsaturated fatty acids in which at least one pair of double bonds and separated by a single bond between them). The main dietary sources of CLA are meat and dairy. Interestingly, meats and dairy sources from grass-fed animals have been found to contain significantly more CLA than what is sourced from grain-fed animals [22]. Bottom line, go with grass-fed.
Hydrogenated Fats
These are unsaturated fats that are highly processed to become solid at room temperature in order to protect against rancidity. Hydrogenation simple describes the addition of hydrogen atoms to molecules, and converts liquid vegetable oils into solid or semi-solid. These types of fats are nearly in every dessert and bakery product known to man, including processed foods such as cookies, crackers, and margarine. Further, solid or semi-solid fats are favored for baking due to the way the fat combines with flour, producing a more suitable texture in the baked product. In addition, partially hydrogenated vegetable oils are cheaper than animal source fats, which makes them very appealing in saving costs but also exhibit other characteristics including increased oxidative stability, or longer shelf life.
Trans Fatty Acid
These types of fats are formed during the process of hydrogenation. Trans fat can be found in numerous processed foods including desserts, microwave popcorn products, frozen pizza, margarine and coffee creamer. It has been linked to an increased risk of heart disease. Although we could discuss this specific fat until your next strength contest, for the most part, trans fatty acids have been shown to increase LDL cholesterol and lower HDL cholesterol, and is a very powerful promoter of systemic inflammation and increase risk for disease. On a more realistic note, the total matrix of a food is more important than just its fatty acid content in predicting the effect of a food on CVD risk [23]. Further, some issues remain unresolved regarding trans fatty acids and CVD risk factors, and many cities in the US have tried (with some success) to band the use of trans fats in restaurants. However, it would be wise to try and avoid these types of fats as best as possible.
Face The Fats
From a historical perspective, humans consumed a variety of meats including bison, buffalo, wild pig, elk, deer, and antelope. In today’s culture we intake considerable more polyunsaturated fats. Not surprisingly, the composition of these animals was very high in saturated and monounsaturated fats, and extremely low in polyunsaturated fats. Renowned researcher Jeff Volek stated the following even 10 years ago from 2005 [24].
“The recommendation to intentionally restrict saturated fat is unwarranted and only serves to contribute to the misleading rhetoric surrounding the health effects of saturated fat.”
Based on years of scientific evidence, it’s safe to say there has never been solid evidence for the idea that these fats cause disease. A meta-analysis published in 2010 looked at 21 studies with a total of 347,747 individuals showed that there is no significant evidence for concluding that dietary saturated fat is associated with an increased risk of CVD[25]. If saturated fats caused heart disease, those individuals who eat more saturated fats should be at far greater risk. But they aren’t. Unfortunately, many people have been brainwashed to believe this as a pure cause and effect relationship due to nutrition policy being wrecked over the past half-century created by a assortment of personal ambition among unscrupulous scientists, bad science, politics and bias. The reality is that fat doesn't make you fat, lazy, slow, weak, diabetic, or sloth-like. It actually helps. For example, in terms of fat loss, studies consistently show that diets that are high in fat (but low in carbs) lead to significant more weight loss compared with low-fat diets [26-28]. Towards the fat loss aim, displacing carbohydrates by increasing fat sets creates an optimal fat-loss environment, as insulin is kept low, aiding in fat usage for energy provisions during training (although a whole different topic). From a physiological and biochemical view, low-fat diets make little sense. Lower-fat diets can also have negative impacts on adipokines (hormones released specifically from your fat cells) which effect fat loss.

It helps to mention that observational studies alone merely demonstrate correlation. So we can’t acquit saturated fat based on such studies alone. Further, the Women’s Health Initiative is the largest randomized controlled trial on diet in history. In this study, 48,835 postmenopausal women were randomized into a low-fat diet group and a control group who continued to consume the standard western diet. After a period of eight years, there was no difference in the rate of cardiovascular disease between the two groups [29, 30]. Other studies also found lower fat diets were not favorable for weight loss, breast cancer, or colorectal cancer[31-33].
So, if we know this, and considering the overwhelming majority of science supports consuming more fats (although methodological difference due exist), still many Americans gravitate towards low fat products, and continue to follow the low-fat guidelines. During the “low fat mythology” on the late 80’s and 90’s, the food industry saw the low-fat, high-carb mantra as an easy opportunity to create a whole new array of products, literally creating a “low fat” food network and designing the “take out the fat and add lots of sugar” formula. How’s that working for you now, people? I’m not going to sit here and blame carbs for everything for the increased health problems facing our nation today, because that’s not entirely true either, as many athletes in a variety of sports consume carbs, both for added fuel and recovery. The problem lies in the corrupt mentality of “good/bad ways of thinking” that all fat is good, all fat is bad; all carbs are good, all carbs are bad. The reality is there are healthy carbs and unhealthy carbs, there's healthy fat and unhealthy fat. I know it’s an oversimplification, but it’s important to maintain context.
Obesity is at an all-time high, and numerous governmental agencies, health and fitness personalities, and even dietitians still don’t understand and accept the veracity of consuming fats and the plethora of benefits they provide. Unfortunately, efforts to reduce the intake of fat are one of the most unfortunate unintended consequences to our society in the history of food and nutrition.
References
- Keys, A., Atherosclerosis: a problem in newer public health. J Mt Sinai Hosp N Y, 1953. 20(2): p. 118-39.
- (ed), A.K., Seven Countries: A multivariate analysis of death and coronary heart disease,. 1980.
- Horowitz, J.F. and S. Klein, Lipid metabolism during endurance exercise. Am J Clin Nutr, 2000. 72(2 Suppl): p. 558S-63S.
- Ormsbee, M.J., et al., Fat metabolism and acute resistance exercise in trained men. J Appl Physiol (1985), 2007. 102(5): p. 1767-72.
- Sareen S. Gropper, J.L.S., Advanced Nutrition and Human Metabolism. 6th ed. 2012, Cengage Learning; 6 edition.
- Farrell, J., Caiozzo, ACSM's Advanced Exercise Physiology 2nd ed. 2012: Lippincott Williams & Wilkins.
- Larson-Meyer, D.E. and K.S. Willis, Vitamin D and athletes. Curr Sports Med Rep, 2010. 9(4): p. 220-6.
- Larson-Meyer, E., Vitamin D supplementation in athletes. Nestle Nutr Inst Workshop Ser, 2013. 75: p. 109-21.
- Todd, J.J., et al., Vitamin d: recent advances and implications for athletes. Sports Med, 2015. 45(2): p. 213-29.
- Davidson, M.H., et al., Clinical utility of inflammatory markers and advanced lipoprotein testing: advice from an expert panel of lipid specialists. J Clin Lipidol, 2011. 5(5): p. 338-67.
- Voight, B.F., et al., Plasma HDL cholesterol and risk of myocardial infarction: a mendelian randomisation study. Lancet, 2012. 380(9841): p. 572-80.
- Feart, C., C. Samieri, and P. Barberger-Gateau, Mediterranean diet and cognitive health: an update of available knowledge. Curr Opin Clin Nutr Metab Care, 2015. 18(1): p. 51-62.
- Garcia-Fernandez, E., et al., Mediterranean diet and cardiodiabesity: a review. Nutrients, 2014. 6(9): p. 3474-500.
- Huo, R., et al., Effects of Mediterranean-style diet on glycemic control, weight loss and cardiovascular risk factors among type 2 diabetes individuals: a meta-analysis. Eur J Clin Nutr, 2014.
- Kien, C.L., et al., Substituting dietary monounsaturated fat for saturated fat is associated with increased daily physical activity and resting energy expenditure and with changes in mood. Am J Clin Nutr, 2013. 97(4): p. 689-97.
- Dorgan, J.F., et al., Effects of dietary fat and fiber on plasma and urine androgens and estrogens in men: a controlled feeding study. Am J Clin Nutr, 1996. 64(6): p. 850-5.
- Sallinen, J., et al., Relationship between diet and serum anabolic hormone responses to heavy-resistance exercise in men. Int J Sports Med, 2004. 25(8): p. 627-33.
- Ellulu, M.S., et al., Role of fish oil in human health and possible mechanism to reduce the inflammation. Inflammopharmacology, 2015.
- Kaur, N., V. Chugh, and A.K. Gupta, Essential fatty acids as functional components of foods- a review. J Food Sci Technol, 2014. 51(10): p. 2289-303.
- Calder, P.C., n-3 polyunsaturated fatty acids, inflammation, and inflammatory diseases. Am J Clin Nutr, 2006. 83(6 Suppl): p. 1505S-1519S.
- Simopoulos, A.P., Evolutionary aspects of diet, the omega-6/omega-3 ratio and genetic variation: nutritional implications for chronic diseases. Biomed Pharmacother, 2006. 60(9): p. 502-7.
- Dhiman, T.R., et al., Conjugated linoleic acid (CLA) content of milk from cows offered diets rich in linoleic and linolenic acid. J Dairy Sci, 2000. 83(5): p. 1016-27.
- Michas, G., R. Micha, and A. Zampelas, Dietary fats and cardiovascular disease: putting together the pieces of a complicated puzzle. Atherosclerosis, 2014. 234(2): p. 320-8.
- Volek, J.S. and C.E. Forsythe, The case for not restricting saturated fat on a low carbohydrate diet. Nutr Metab (Lond), 2005. 2: p. 21.
- Siri-Tarino, P.W., et al., Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. Am J Clin Nutr, 2010. 91(3): p. 535-46.
- Santos, F.L., et al., Systematic review and meta-analysis of clinical trials of the effects of low carbohydrate diets on cardiovascular risk factors. Obes Rev, 2012. 13(11): p. 1048-66.
- Hession, M., et al., Systematic review of randomized controlled trials of low-carbohydrate vs. low-fat/low-calorie diets in the management of obesity and its comorbidities. Obes Rev, 2009. 10(1): p. 36-50.
- Westman, E.C., et al., Low-carbohydrate nutrition and metabolism. Am J Clin Nutr, 2007. 86(2): p. 276-84.
- Howard, B.V., et al., Low-fat dietary pattern and weight change over 7 years: the Women's Health Initiative Dietary Modification Trial. JAMA, 2006. 295(1): p. 39-49.
- Krauss, R., Low-fat dietary pattern and risk of cardiovascular disease in the Women's Health Initiative Randomized Controlled Dietary Modification Trial. Curr Atheroscler Rep, 2007. 9(6): p. 431-3.
- Beresford, S.A., et al., Low-fat dietary pattern and risk of colorectal cancer: the Women's Health Initiative Randomized Controlled Dietary Modification Trial. JAMA, 2006. 295(6): p. 643-54.
- Prentice, R.L., et al., Low-fat dietary pattern and risk of invasive breast cancer: the Women's Health Initiative Randomized Controlled Dietary Modification Trial. JAMA, 2006. 295(6): p. 629-42.
- Howard, B.V., et al., Low-fat dietary pattern and risk of cardiovascular disease: the Women's Health Initiative Randomized Controlled Dietary Modification Trial. JAMA, 2006. 295(6): p. 655-66.


9 Comments