




- Thank you for asking Dave injury questions, because it helps me help you.
- Hang with me on some background here — the more you know, the better equipped you will be in the future.
RECENT: Keyboard Warriors Need to Stop!
Having also suffered a relatively severe groin injury with no surgical options and poor prognosis and watching a friend of mine incur a similar one (and all three of us have had relatively different healing speeds and results), it’s clearly worth delving into at least a bit in terms of pathology, development, and how to go about working through and rehabbing groin injury, as well as what other factors may come into play with regards to either return to sport or getting back under a bar. A very smart person recently told me that people read articles because they want to know “how” to accomplish their goal or get to a certain point; Dave’s injury questions, I think, are an illustration of that. And for me to help you get to your “how to get through a groin injury” answer, there are a few basic things to be understood first.
I don’t want to say that the exploration of groin injury has become a more researched topic in more recent years because it may just be that my exposure to it has increased, but it does seem that as our paradigm shifts from a strictly biomechanical model to a multifaceted neurophysiological approach (read: our nervous system adapts) to orthopedic or sports-related injury, groin injuries, in particular, have gotten a bit more of the limelight; they’re sensitive injuries that, though purely anecdotally seen in practice across years of patients, seem to be especially prone to high degrees of irritability and sensitivity despite normal and appropriate healing processes.

With the high prevalence of things like FAI, adductor strains/tears, and general joint wear and tear, it’s important to acknowledge that while some of what worked for training partners dealing with those issues may work for you, it’s worth it to seek the cause, your “why,” rather than jumping from one exercise or idea to the next. I told myself to write down potential pain generators in the hip and groin and to stop as soon as I had to think for more than a few seconds. Here’s the list I came up with, quick and dirty, in absolutely no particular order:
- Hip impingement
- Endometriosis (I had a patient that responded to nothing I did with her clinically — referred her on and good thing!)
- Inguinal hernia
- Developmental/congenital abnormalities (SCFE, dysplasia related disorders, tissue disorders)
- Labral tear
- Fracture (multiple types)
- Abdominal hernia
- High hamstring strain (truthfully, this is one of the places I feel my pain the most after my injury)
- Visceral (e.g., organ-related) pain
- Pelvic floor pain/dysfunction (especially in a population that lifts frequently and employs Valsalva strategies)
- Intra-articular (true hip joint) pathology or degeneration (osteoarthritis)
- Nerve entrapment
- Lumbar spine or sacroiliac regional referral
- Muscle tear
- Avulsion fracture
- Athletic pubalgia
- Tendon rupture
Subclassification to localized (e.g., non-referral, non-visceral):
- Hip impingement
- Inguinal hernia
- Developmental abnormalities (SCFE, dysplasia-related disorders)
- Labral tear
- Fracture (multiple types)
- High hamstring strain
- Pelvic floor pain/dysfunction (especially in a population that lifts frequently and utilizes Valsalva maneuvers)
- Intra-articular (true hip joint) pathology or degeneration (osteoarthritis)
- Nerve entrapment
- Muscle tear
- Avulsion fracture
- Athletic pubalgia
- Tendon rupture
RELATED: Femoro-Acetabular Impingement and the Rehab Process: The Diagnosis
On a HUGE assumption here as iron sports athletes, for the sake of simplicity, let’s chuck all the weird internal or pelvic stuff out the window. We could further classify these injuries to traumatic versus chronic, and it’d hit the nail on the head for most people actually interested in this article — the people interested in Dave’s answer: How do I move forward after this? Which really is asking the question, “Is my best behind me/will I lift heavy again?” And still, I’m going to bring you back to the list above and highlight that there are different tissues affected by the above-mentioned possibilities, even the traumatic ones: tendon, muscle, bone, and cartilage.
The time it takes for you, a training partner, or your athlete to heal is going to depend completely on what type of tissue was affected (sometimes, more than one), as well as a constellation of other mechanisms that seem to either crank up or down the overall irritability and sensitivity of the area.

There is actual science to this, rather than just chasing endless mobility drills from social media and hopping under a bar to squat as the end goal. This science is based on cell biology and tissue type, and we have GOT to appreciate that, but what more and more studies continue to show is that the healing and treatment of tissue (tendon, especially) is only moderately understood and often multifactorial from more than the histology or types of cells approach.
I wish I’d saved the article, but I remember recently reading a sentence along the lines of, “We are only beginning to understand the neurophysiological mechanisms of groin injury.” I’ve got multiple examples off the top of my head all with varying recovery times, varying severity of injury, and varying tissue types involved that I’ll be going through in an upcoming series for groin injury rehab. There are quite a few parallels and major themes that emerge, if you will, but also themes of things we neglect as athletes because I’m like you: I want to get back under the bar as soon as possible.
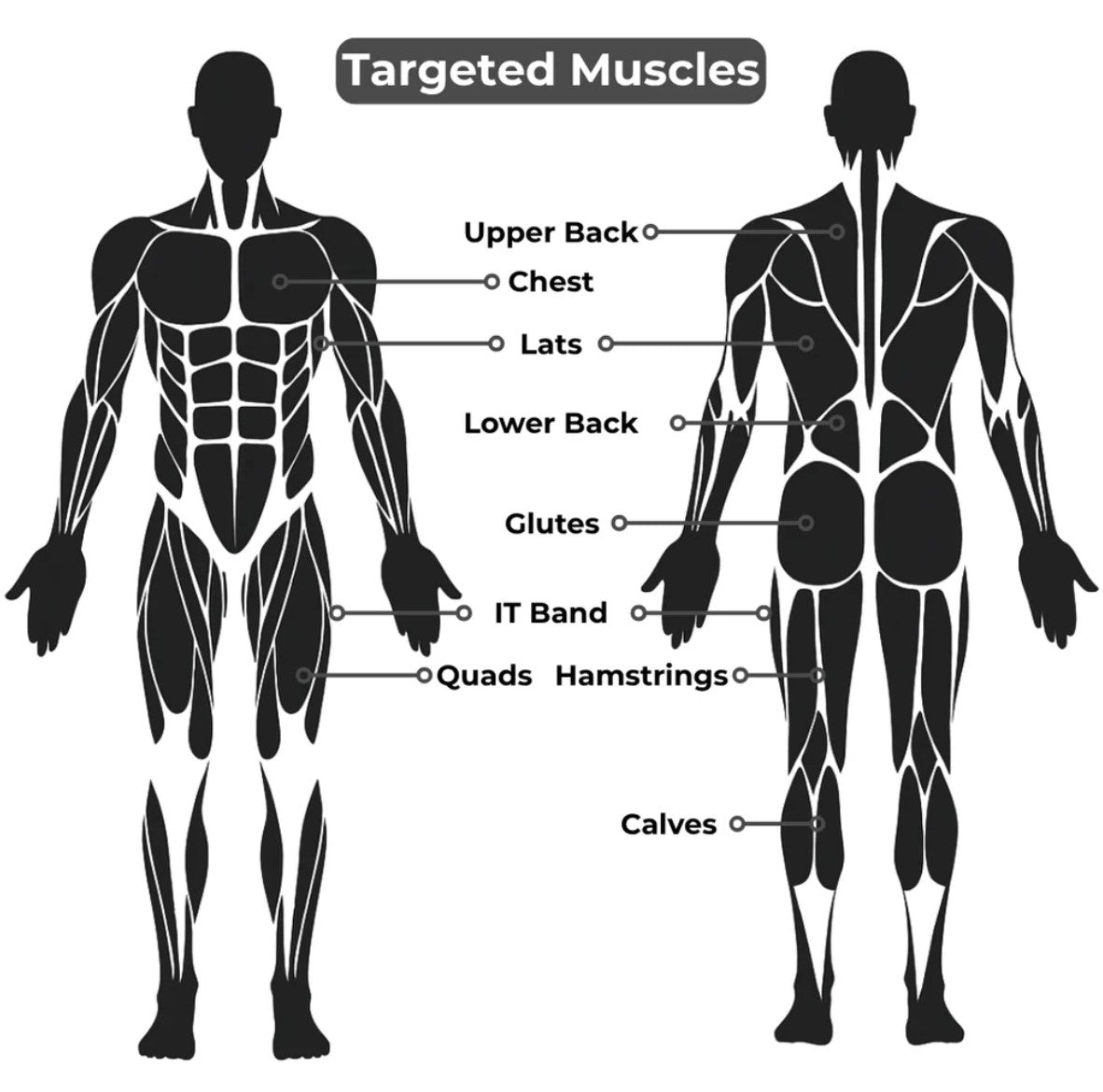
Any traditional rehab program or protocol is going to emphasize low ab and glute training in varying ranges of motion. And that’s a great start — but given that’s well-known, I want to use this series to give you a little something different to think about. Prior to understanding the biology of groin injuries, understanding the anatomical importance of the involved musculature is paramount with an understanding that position determines function. Every time you look at an anatomy diagram, I would challenge you to think about how lines of pull, mechanical advantage, and subsequent actions may shift as the body shifts, because it does and it will.
When it comes to surrounding and stabilizing a ball and socket joint that’s constantly moving or stabilizing in three planes, ultimately leading to whatever the etiology of our groin pain is from the long list above, it’s important to actually stop and consider what is happening as the joint and respective musculature changes position, as the joint moves, and what ultimately is happening to the affected tissue (which will vary by diagnosis) with movement. From there, breaking down principles such as range of motion, load, dosage, among others, is what is going to get you back to training. Muscle is going to handle that much different than tendon, which both differ from the ever-common impingement and associated labral issues.
READ MORE: Troubleshooting Strength Injuries: Dealing with Injury
Let’s use the glute max as an example with an adductor longus tear (which is what Dave had). The principles of agonist/antagonist muscle groups are commonly thought of in one, occasionally two, planes of motion, depending on the muscles utilized. We think biceps/triceps, quads/hamstrings, and easy uni-planar pairs. We don’t often think about the glute complex being an antagonist to the adductor group, but especially in certain ranges of motion, the two groups work to stabilize the pelvis in the frontal and transverse plane. Given that pain is generally an inhibitory response after injury, the role of neuromuscular inhibition may contribute to decreased ability to generate proprioceptive awareness of a contraction, decreased multi-section coordination (the glute max has three distinct ones), and a protectively oriented decrease in control.
We know what a glute does and we know what an adductor does; both play a role in controlling the femur, which is how we think about them. If we take this a step further (which is what I’d encourage you to do) and keep the femur “fixed,” they also work to stabilize and control the pelvis. This is where I see the biggest need for deviation from standard run-of-the-mill rehab programs and textbooks. While they’re great resources, they’re not going to hit a home run on adapting to YOUR body and figuring out where you don’t fit the textbook, because I guarantee at some point you won’t, and you might need to think a little outside of the box to do so.
What I want to offer you in the next series is an appreciation for the role of anatomy beyond a textbook that’s rehab-dependent on what YOU need and to offer some basic starting points and ideas to chew on. I cannot (read: will not) write a protocol or firm progression unless you and I have consulted individually, but I am a firm believer in that the more you know about why different injuries respond the way they do, the less time you’ll spend spinning in circles, and the more time you’ll spend actually working back toward what you love and the less chaotic the injury will feel.
Thank you for asking Dave about his injuries because when you ask questions, it helps us (read: me) answer. If there are a few of you dealing with groin injuries, it’s worth making a series about, as the umbrella of groin injury is broad, and what you need might be different than what Dave needed based on structures involved. I certainly hope you handle it differently than he did. I’m not going to lie, I’ve had a number of injuries through my training, but Dave was right: groin injuries are a different beast, and the nature of the beast is going to depend more fully on what actual tissue was affected.
Part 2: A Muscle Tear
Part 3: Tendon Injuries