









In the first part of this article, we examined the forces placed on a young athlete through strength training. Through multiple scientific formulas, we demonstrated that the forces placed on an athlete through running, jumping, cutting, and other athletic movements is significantly higher than the forces placed on an athlete through weight training.
In this second part, we are going to look at more research regarding 1RM testing and break down multiple falsehoods about why young athletes should not strength train.
What does the research say about the relative safety of weight training and children?
So we’ve heard it time and time again from coaches, parents, and “professionals” that weight training will injure your children.
- Children should not strength train. It is dangerous and hazardous. It usually goes something like this: if you strength train your kid, they’ll be FUBAR!
- You can’t have children lift heavy weights or 1 RM’s because it will cause structural damage.
- If you strength train young athletes, you will injure their growth plates and stunt their growth.
- Children can’t get strong because they don’t produce enough testosterone.
So what does the research say about the above comments that we hear about every day?
There is no statistically convincing evidence in the scientific literature that weightlifting or weight training are particularly hazardous. The overwhelming impression from the surveys and literature is that both are markedly safer than many other sports, certainly when supervised by qualified people (8).
Findings from the 2012–2013 High School Sports-Related Injury Surveillance Study revealed that participation in team sports resulted in an estimated 1.36 million injuries at a rate of 2.16 injuries per 1,000 athlete exposures (i.e., practices and competition). Of the nine sports studied, football had the highest injury rate (3.87 injuries per 1,000 athlete exposures), whereas boys’ baseball (0.88) and girls’ softball (0.89) had the lowest injury rates (9).
Data comparing the relative safety of resistance training, weightlifting, and other sports are limited. In a retrospective evaluation of injury rates in adolescents, it was revealed that resistance training and weightlifting were markedly safer than many other sports and activities. In this report, the overall injury rate per 100 participant hours was 1.92 for rugby and 0.0027, 0.0120 and 0.0013 for powerlifting, resistance training and weightlifting, respectively. (8)
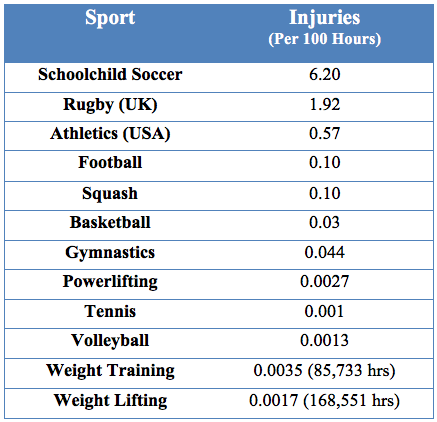
Multi-Sports Comparative Injury Rates (Hamill, 1994)
A study published in the November/December 2001 issue of the Journal of American Academy of Orthopaedic Surgeons cited research showing that in children ages five to 14 years, the number of injuries from bicycling was almost 400 percent greater than the number of injuries from weightlifting (10).
In a review paper on resistance training for prepubescent and adolescents published in 2002 in Strength and Conditioning Coach, author Mark Shillington reported in a screening of sports‐related injuries in school-aged children that resistance training was the likely cause of only 0.7 percent (or 1,576) of injuries compared with 19 percent for football and 15 percent for baseball (11).
Dr. Avery Faigenbaum, one of the leading research scientist in the children and strength training field, has reported that for over 17 years he and colleagues conducted strength training classes for children, ages six to 12, without a single injury.
The truth is that weight training and competitive lifting sports are among the safest activities an athlete can participate in. This fact is known worldwide. Renowned Russian sports scientist Vladimir Zatsiorsky in his book “Science and Practice of Strength Training” states, “The risk of injury from a well coached strength training program has been estimated to be about one per 10,000 athlete‐exposures, with an athlete‐exposure being defined as one athlete taking part in one training session or competition. Compared to tackle football, alpine skiing, baseball pitching, and even sprint running, strength training is almost free of risk.” (12)
What does the research tell us about 1RM testing for young athletes?
Another area of potential injury concern for children and pubescent/adolescents is the use of max testing (1RM). The argument that weightlifting is inherently more dangerous than weight training because it involves single, maximum efforts implies that other sports, considered safer, do not. In fact, jumping, kicking, striking, tackling, and throwing are often single maximum efforts. The last repetition of a set in weight training is frequently a maximum effort. (8)
Most of the forces that youth are exposed to in various sports and recreational activities are likely to be greater in both exposure time and magnitude than competently supervised and properly performed maximal strength tests. These observations along with current research findings indicate that the maximal force–producing capabilities of healthy children and adolescents can be safely evaluated by 1RM testing procedures, provided that youth participate in a habituation period before testing to learn proper exercise technique, and qualified professionals closely supervise and administer each test (4).
Some clinicians and researchers have not used 1RM testing to evaluate training-induced changes in muscular strength because of the presumption that high-intensity loading may cause structural damage in children. Thus, the maximal force production capabilities of children have not been directly evaluated in some studies, yet no injuries have been reported in prospective studies that utilized adequate warm-up periods, appropriate progression of loads, close and qualified supervision, and critically chosen maximal strength tests (1RM performance lifts, maximal isometric tests, and maximal isokinetic tests) to evaluate resistance training–induced changes in children (4). In a study, 96 children performed a 1RM strength test on one upper-body and one lower-body weight machine exercise. No abnormal responses or injuries occurred during the study period, and the testing protocol was reportedly well tolerated by the subjects (13). In other reports, children and adolescents safely performed 1RM strength tests using free weight exercises (14, 15, 16, 17, 18, 19, 20, 21, 22, 23). Faigenbaum and others have shown max testing to be safe in these age groups (4, 24, 25).



It should be noted that researchers emphasize that when performing 1RM max testing, maintaining technique is critical. A multi-rep max (e.g., 3 – 5 RM) may even be preferred to a 1RM in certain situations, especially where training age (i.e. number of years experience in resistance training) is less than three to four years or physical development is behind what is expected for the chronological age (4). They also recommended that NSCA-prescribed guidelines for lifting technique should always be followed (26).
But you'll injure their growth plates and stunt their growth!
Although children and adolescents are susceptible to injury to the growth cartilage, the potential for this type of injury may be less in a preadolescent child than in an adolescent because the growth cartilage may actually be stronger and more resistant to sheering type forces in younger children (4, 27). To date, injury to the growth cartilage has not been reported in any prospective youth resistance training research study. Furthermore, there is no evidence to suggest that resistance training will negatively impact growth and maturation during childhood and adolescence (4, 28, 29).
Malina examined the effects of resistance training programs on pre- and early-pubertal youth in the context of response, potential influence on growth and maturation, and occurrence of injury. The estimated injury rates were 0.176, 0.053, and 0.055 per 100 participant-hours in the programs. These extremely low injury rates were attributed to the high levels of supervision and low instructor to participant ratios. They concluded that weights and resistance machines and with supervision and low instructor/participant ratios are relatively safe and do not negatively impact growth and maturation of pre- and early-pubertal youth (30).
Mel Siff in Facts and Fallacies of Fitness states, “It has never been shown scientifically or clinically that the periodic imposition of large forces by weight training on the growing body causes damage to the epiphysial plates." Siff also notes that bone density scans have proven that youngsters who do competitive weightlifting (i.e., the snatch and the clean and jerk) have higher bone densities than children who do not use weights, and that clinical research has not shown any correlation between weight training and epiphysial damage (7).
As far as stunting a child’s growth, there is no current evidence to indicate a decrease in stature in children who regularly strength train in a supervised environment with qualified instruction. In all likelihood, participation in strength training will have a favorable influence on growth at any stage of development but will not affect a child’s genetic height potential (31).
MORE: How To Develop Strength in Untrained Children
As with muscles, bones become stronger in response to stress, and the activities involving the highest levels of stress can encourage the formation of stronger bones. An extensive Russian study on young athletes, published in a book entitled School of Height, concluded that heavy lifting tends to stimulate bone growth in young athletes rather than inhibit it. (32)
Children cannot increase strength through strength training because they do not produce enough testosterone
Testosterone is not essential for achieving strength gains, as evidenced by women and elderly individuals who experience impressive gains in strength even though they have little testosterone. When compared on a relative or percent basis, training-induced strength gains in children are comparable to those in adolescents and adults (31). You are fooling yourself if you think your child can’t get stronger.
Conclusion
It should be a no-brainer that young athletes embrace strength training. The benefits of strength training will yield bigger and stronger bones, tendons, ligaments and muscles. These benefits allow the body to be more resistant to all of the external forces and demands being placed upon it in athletic sports training and lower the possibility of injury.
Meanwhile at Competitive Edge APC….
At our facility when we begin working with an athlete, the primary focus is on good technique. Once proper form and technique is established, we load our athletes and get them strong. What we’ve seen through training our athletes throughout the years is that it takes a good three years of consistent strength training to build a solid foundation of strength. This is the point that we see in our athletes training where the muscles, bones and connective tissues (tendons, ligaments) really start getting strong and when our athletes start hitting impressive numbers on ALL performance measures.
When we hear parents, coaches, therapists and others telling their athletes not to strength train because they are afraid the strength training will hurt them or because they’ll become bulky and slow, we laugh. We know when our athletes meet on the field, ours will be running right through yours! When our 6-foot, 225-pound fullback who power cleans 250 pounds, bench presses 325 and squats 450 faces off against your 155-pound linebacker with no weight training experience, things will not end well for the other guy.
If your child is participating in a speed school/camp because you’re afraid that weightlifting is going to hurt your child, you’ve been sold a line by some weak, nimble-armed shyster. You’re now armed with the facts why strength training is not only safe, but probably the most important thing you can do to protect your child from injury.
Unfortunately, we do not have enough competent strength coaches nor do we have any standards for someone to call themselves a strength coach. Because of this, the uneducated continue to promote the idea that strength for training young athlete is a wrong and that it will hurt them and stunt their growth. Armed with the above information, it’s up to people to call these people out and educate them not only the benefits of strength training but the sheer necessity of it to protect them from injury when they begin playing at higher levels.
References
- Micheli L. Preventing Injuries In Sports: What The Team Physician Needs To Know. In: Chan K, Micheli L, Smith A, Rolf C, Bachl N, Frontera W, Alenabi T, Eds. F.I.M.S. Team Physician Manual, 2nd Ed. Hong Kong: CD Concept; 555-572, 2006.
- PEDIATRICS. American Academy Of Pediatrics. Committee On Sports Medicine. Strength Training By Children And Adolescents. Vol. 107 No. 6 June 2001June 2001.
- American College Of Sports Medicine (ACSM). Current Comment 'Youth Strength Training.' March 1998.
- Faigenbaum, Avery D., Et Al. "Youth Resistance Training: Updated Position Statement Paper From The National Strength And Conditioning Association." Journal Of Strength And Conditioning Research 23.5 (2009): S60-S79.
- American College Of Sports Medicine (ACSM). "The Prevention Of Sports Injuries Of Children And Adolescents." Medicine & Science In Sports & Exercise, 1993, 25 (8, Supplement), 1-7.
- Micheli, L.J. Physiological and orthopaedic considerations for strengthening the prepubescent athlete. Nat. Strength Condo Assoc. J. 7(6):26-27.1986
- Siff, M.C. (2003). Facts and Fallacies of Fitness. Denver: Supertraining Institute.
- Hamill, B. Relative safety of weight lifting and weight training. J Strength Cond Res 8: 53–57, 1994.
- Centers for Disease Control and Prevention. Sports-related injuries among high school athletes—United States, 2005–06 school year. MMWR Morb Mortal Wkly Rep 55: 1037–1040, 2006.
- J.M. Purvis, R.G. Burke. (2001). Recreational Injuries in Children: Incidence and Prevention . J Am Acad Orthop Surg. Nov-Dec;9(6):365-374.
- Shillington, M. (2002). Resistance Training For Prepubescents And Adolescents: A Review. Strength and Conditioning Coach. (Vol. 9, No. 3).
- Zatsiorsky, V.M. (1995). Science and practice of strength training. Champaign, IL: "Human kinetics"
- Faigenbaum, A, Milliken, L, and Westcott, W. Maximal strength testing in children. J Strength Cond Res 17: 162–166, 2003.
- Baker, D. Differences in strength and power among junior-high, senior-high, college-aged, and elite professional rugby league players. J Strength Cond Res 16: 581–585, 2002.
- Benson, A, Torade, M, and Fiatarone Singh, M. A rationale and method for high-intensity progressive resistance training with children and adolescents. Contemp Clin Trials 28: 442–450, 2007.
- Hetzler, R, DeRenne, C, Buxton, B, Ho, K, Chai, D, and Seichi, G. Effects of 12 weeks of strength training on anaerobic power in prepubescent male athletes. J Strength Cond Res 11: 174–181, 1997.
- Horvat, M, Franklin, C, and Born, D. Predicting strength in high school women athletes. J Strength Cond Res 21: 1018–1022, 2007.
- Kravitz, L, Akalan, C, Nowicki, K, and Kinzey, S. Prediction of 1 repetition maximum in high school power lifters. J Strength Cond Res 17: 167–172, 2003.
- Mayhew, J, Kerksick, C, Lentz, D, Ware, J, and Mayhew, D. Using repetitions to predict one-repetition maximum bench press in male high school athletes. Pediatr Exerc Sci 16: 265–276, 2004.
- Mayhew, J, McCormick, T, Piper, F, Kurth, A, and Arnold, M. Relationships of body dimensions to strength performance in novice adolescent male powerlifters. Pediatr Exerc Sci 5: 347–356, 1993.
- Ozmun, J, Mikesky, A, and Surburg, P. Neuromuscular adaptations following prepubescent strength training. Med Sci Sports Exerc 26: 510–514, 1994.
- Sadres, E, Eliakim, A, Constantini, N, Lidor, R, and Falk, B. The effect of long-term resistance training on anthropometric measures, muscle strength, and self-concept in pre-pubertal boys. Pediatr Exerc Sci 13: 357–372, 2001.
- Volek, J, Gomez, A, Scheett, T, Sharman, M, French, D, Rubin, M, Ratamess, N, McGuigan, M, and Kraemer,W. Increasing fluid milk intake favorably affects bone mineral density responses to resistance training in adolescent boys. J Am Diet Assoc 103: 1353– 1356, 2003.
- Faigenbaum A.D., Kraemer W.J., et al./NATIONAL STRENGTH & CONDITIONING ASSOCIATION. Youth resistance training: position statement paper and literature review. Strength & Conditioning 18(6): 62 – 75, 1996.
- Faigenbaum A.D., Micheli L.J./AMERICAN COLLEGE OF SPORTS MEDICINE. Current Comment from the American College of Sports Medicine: Youth Strength Training. Indianapolis IN: ACSM, 1998
- Baechle T.R., Earle R.W. (Editors)/ NATIONAL STRENGTH & CONDITIONING ASSOCIATION. Essentials of Strength Training & Conditioning (3rd Edition). Champaign IL: Human Kinetics, 2008.
- Micheli, L. Strength training in the young athlete. In: Competitive Sports for Children and Youth. Brown, E and Branta, C eds. Champaign, IL: Human Kinetics Books, 1988. pp. 99–105.
- Falk, B and Eliakim, A. Resistance training, skeletal muscle and growth. Pediatr Endocrinol Rev 1: 120–127, 2003.
- Malina, R.Weight training in youth-growth, maturation and safety: An evidenced based review. Clin J Sports Med 16: 478–487, 2006.
- Malina, R.M. Weight training in youth growth, maturation and safety: An evidence-based review. Clinical Journal of Sports Medicine 16(6): 478–487, 2006.
- Faigenbaum, AD (2102). Youth Strength Training: Facts and Fallacies. American College of Sports Medicine. http://www.acsm.org/access-public-information/articles/2012/01/13/youth-strength-training-facts-and-fallacies
- Palko, AS. (2007). School Of Height (M. Yessis, Trans.). Michigan: Ultimate Athlete Concepts.
Matt Wattles is the Head Strength and Conditioning Coach and owner of Competitive Edge Athletic Performance Center in Meridian, ID (www.edgemeridian.com). He has a M.S. in Exercise Science and over 20 years in strength and conditioning and is both an athlete and coach/trainer. Matt is a past President of the American Society of Exercise Physiologist (ASEP), has published numerous articles in professional and research journals, and has been an invited presenter at national conferences throughout the country.

I have to ask...is there a part 3?
v/r
Donald
I really like the thorough research that has gone into your piece!
Keep up the great work!